From Connection to Protection — Realizing Every Child's Digital Right to Privacy, Safety, Information, and Health |
juin 25, 2026 . 7 Minutes read
Children's Rights in a Digital World: Evidence-Based Innovation for Babies, Parents, and Communities—from Northwest Cameroon to the Global Stage
Children today are born into a digital environment that shapes their health, learning, safety, and identity from the very first SMS reminder after birth. Grounded in the UN Convention on the Rights of the Child and General Comment No. 25, this article explores how evidence-based digital tools, parenting support, and health systems can turn that environment into a vehicle for protection rather than risk.
From First Cry to First Click: Claiming Children's Rights in a Connected World
A child born today opens eyes in a world woven from screens, signals, and algorithms. By the time her mother brings the baby home from the maternity ward, an SMS may already be reminding the family of the next vaccination appointment. By her first steps, a voice assistant may be answering her earliest questions, and by the time she enters school, her digital footprint is already part of how she is seen, profiled, and served. The Convention on the Rights of the Child, adopted in 1989—long before smartphones and social media—now has to govern a digital environment its drafters could not have foreseen. In 2021, the UN Committee on the Rights of the Child issued General Comment No. 25 to clarify that every right in the Convention must be respected, protected, and fulfilled online, including children's rights to privacy, safety, education, participation, non-discrimination, and the highest attainable standard of health. Yet research shows that implementation still lags behind children's rapidly expanding digital lives, and that decisions about platforms and policy often fail to put children's best interests first. [1-3 & 8]
The question is no longer whether children belong online—they already do—but how to ensure that every child, in every income group and every crisis‑affected community, can exercise their digital rights in practice. That includes the boy in a rural Cameroonian village whose mother cannot read his vaccination card, the displaced family who lost their immunization records to conflict, and the teenager scrolling alone at free time with an AI chatbot as her only companion. [2 &3]
From Bamenda, where mothers navigating instability are reconnected to life‑saving vaccines through a simple SMS and an integrated vaccination app, to global classrooms where children and parents are learning to negotiate AI together, the story of children's digital rights is being written now. CIMA Care—recognized by the United Nations Office on Drugs and Crime (UNODC) for integrating evidence-based parenting guidance into its digital vaccination platform in Cameroon—is proud to help write that story, combining child‑rights principles with practical tools that reach families where they are. [4-8]

From first cry to first click, mothers can connect their baby's right to health via CIMA.
The Two Faces of the Digital World — Opportunity and Risk for Every Child
UNICEF describes today's digital environment as a paradox: it offers children unprecedented opportunities for learning, connection, and play, while simultaneously exposing them to serious risks. As UNICEF's Digital Parenting hub explains, "being online offers so many positives for children – from staying connected with friends and family, to exciting learning opportunities and a wealth of entertainment. But all this new technology can be a lot for anyone to keep up with, and there are risks and worries – from digital privacy to staying safe online and harmful content." [9-11]
Protecting children's digital rights is therefore not a task families can shoulder alone; it is a shared responsibility across governments, technology companies, schools, health systems, and community institutions. Within that wider ecosystem, CIMA Care operates at the most foundational level: upholding the child's right to health from birth and ensuring that digital innovation strengthens rather than undermines that right. [9-10, 12-14]

Opportunity meets risk in every child's digital life—CIMA Care holds the foundational line.
The Digital Divide Is a Children's Rights Issue — and It Is Widest Where Children Are Youngest
UNICEF's State of the World's Children 2024 report highlights a stark reality. In 2024, over 95% of people in high‑income countries are connected to the Internet, compared with only about 26% in low‑income countries. [15]
Because the world's youngest populations are growing fastest in regions with the weakest connectivity—especially across sub-Saharan Africa—this digital divide is poised to deepen existing inequalities in health, learning, and protection, limiting children's life chances precisely where their needs are greatest. [15 & 16]
This inequity has direct health consequences. UNICEF emphasizes that "in many places, especially low-income countries and humanitarian settings, health-sector digitalization is not systematically invested in. This can result in weakened, fragmented systems, create new risks to child wellbeing, and increase burdens on frontline health workers. In these instances, the children most in need are often left behind." [17] The Rwandan transition from "piles of registers to digital care," illustrates what happens when that gap is closed: in a UNICEF‑supported pilot, 600 community health workers received smartphones and began using a community electronic medical records system, and the initiative is now being scaled nationally with tens of thousands of CHWs engaged, demonstrating how last‑mile digital tools can strengthen equity and service quality.[8]
Recent academic evidence confirms the power of well‑designed digital tools for childhood vaccination. A 2025 systematic review of mHealth and digital health interventions across 19 sub-Saharan African countries found that interventions using SMS, voice calls, apps, and other digital tools generally improved vaccination coverage and timeliness, with approaches that included voice components appearing particularly promising, though the certainty of the evidence ranged from very low to moderate. [18]
An earlier 2021 BMJ Global Health meta‑analysis showed that SMS reminders significantly increased childhood immunization coverage (RR = 1.16; 95% CI 1.10–1.21) and the timely receipt of vaccines (RR = 1.21; 95% CI 1.12–1.30), with effects significantly larger in lower‑middle‑ and low‑income countries than in upper‑middle‑income settings. [19]
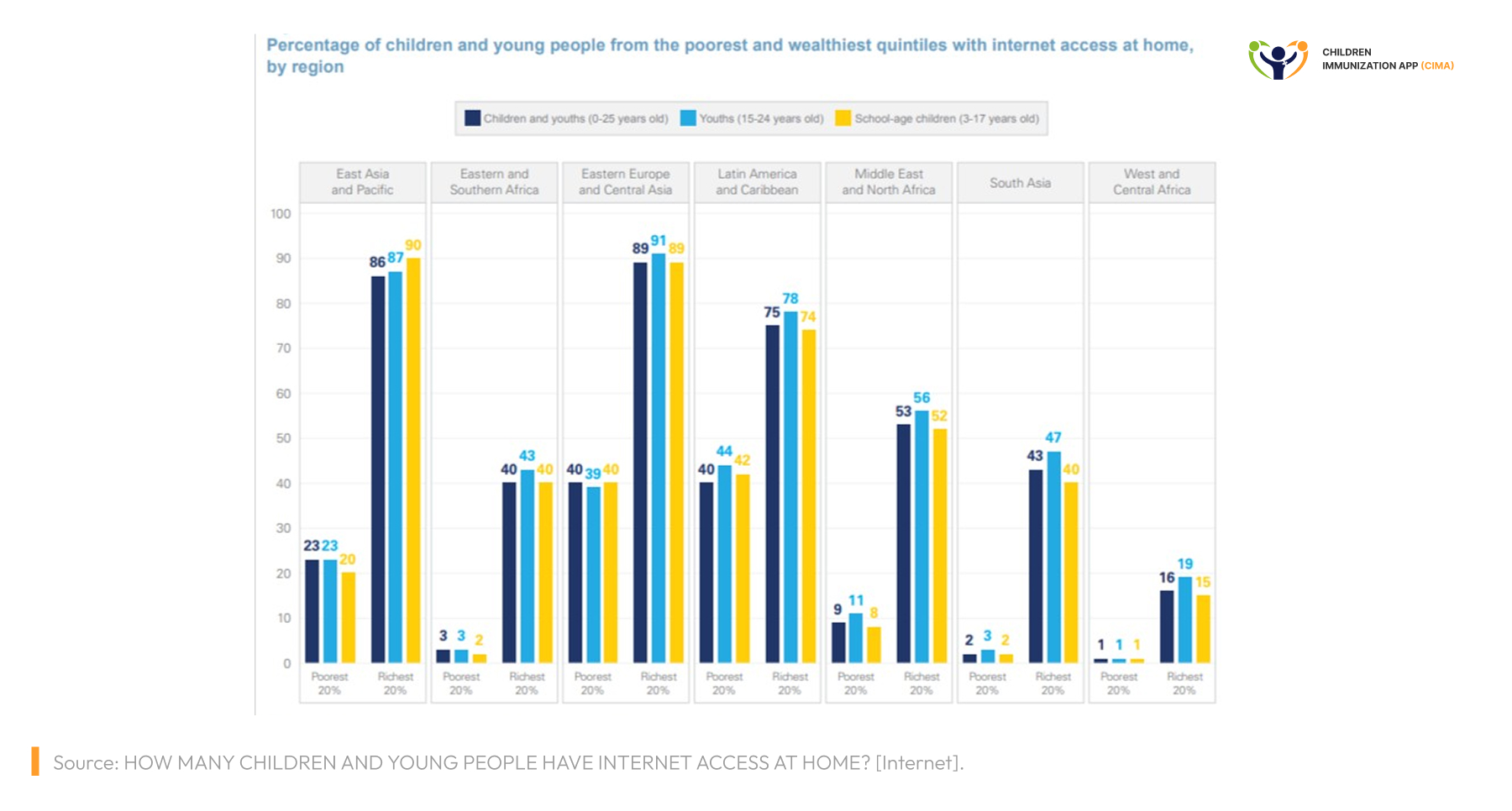
In West Africa's most impoverished homes, 1% of children are online. The digital divide is a rights gap.
The UN's Framework: Privacy, Safety, Participation, and Health Online
General Comment No. 25 (2021) is the global reference point for children's digital rights. It anchors four principles that should structure every digital service touching a child or family:
- Non-discrimination — every child must benefit from digital opportunities equally, regardless of income, language, ability, gender, or geography.
- Best interests of the child — design and policy choices must place the child's wellbeing above commercial interest.
- Right to life, survival, and development — digital systems must support, not undermine, children's physical, mental, social, and emotional growth.
- Respect for the child's views — children must be heard in shaping the digital environment that affects them. [20]
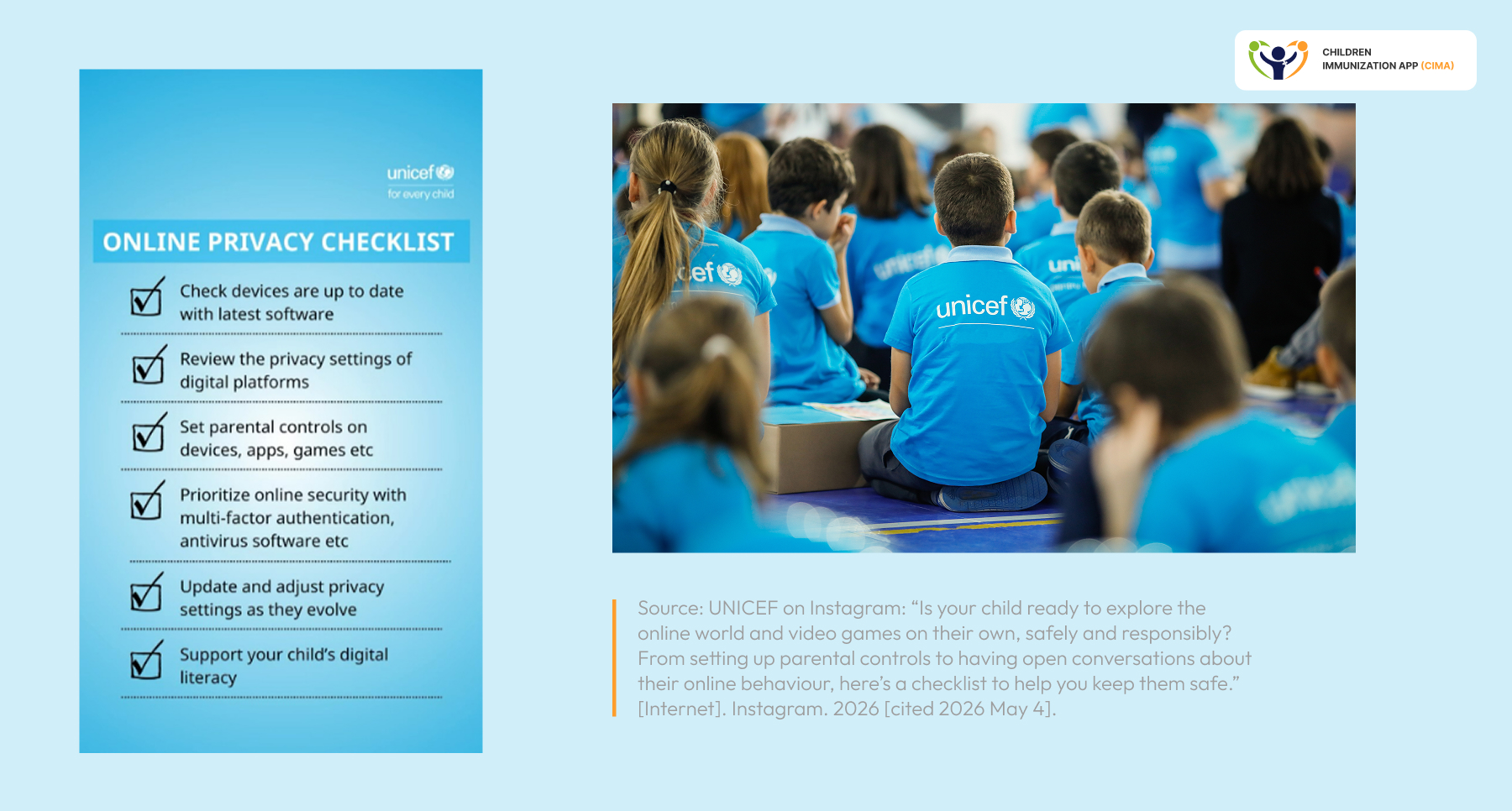
On privacy, UNICEF's Online Privacy Checklist for Parents encourages families to keep devices and software updated, adjust privacy settings, limit app permissions, use parental controls, and talk early with children about their "digital footprint" as part of building lifelong digital literacy—not as a set of fear‑based rules. In parallel, UNICEF’s wider policy guidance on AI and children calls on decision‑makers and developers to follow a responsible data approach, including purpose‑specific and minimal data collection and processing, and to adopt privacy‑by‑design when building systems that affect children. [21]
These principles are not abstract for global health. When CIMA Care's app is used to register a baby's vaccinations and trigger SMS reminders, the same standards apply: data must be minimized, purposes must be transparent, and the family's voice must shape the experience. The UNODC's 2024 recognition of CIMA Care explicitly highlighted that "the integration of UNODC parenting tips into a vaccination app launched in Cameroon (CIMA) was a demonstration of how technology can bridge diverse tools to provide vital support in challenging environments for the benefit of children and families in need."[4-5]
The UN framework—from privacy checklists to children's voices.
New Frontiers of Risk: Mental Health, AI, and Cyberbullying
1. The Mental Health Signal Is Real and Rising
The WHO Regional Office for Europe's 2024 HBSC report on adolescent social media and gaming—drawing on data from almost 280,000 adolescents in 44 countries and regions—found that the proportion of adolescents with problematic social media use rose from 7% in 2018 to 11% in 2022, with girls reporting higher levels than boys (13% vs 9%). [22]
Globally, the WHO estimates that around 1 in 7 adolescents aged 10–19 years lives with a mental disorder, accounting for roughly 13–15% of the disease burden in this age group. [20 & 23-24]
These figures matter for any organization serious about children's rights, because Article 24 of the Convention on the Rights of the Child guarantees the highest attainable standard of health, and mental health is part of that right. Healthcare workers, parents, and community health workers are often the first to spot warning signs. UNICEF's parenting materials describe these as withdrawal, changes in sleep or appetite, distress or agitation after being online, and unusual secrecy about digital activity, and advise adults to respond with calm, open conversations and practical support. [25]
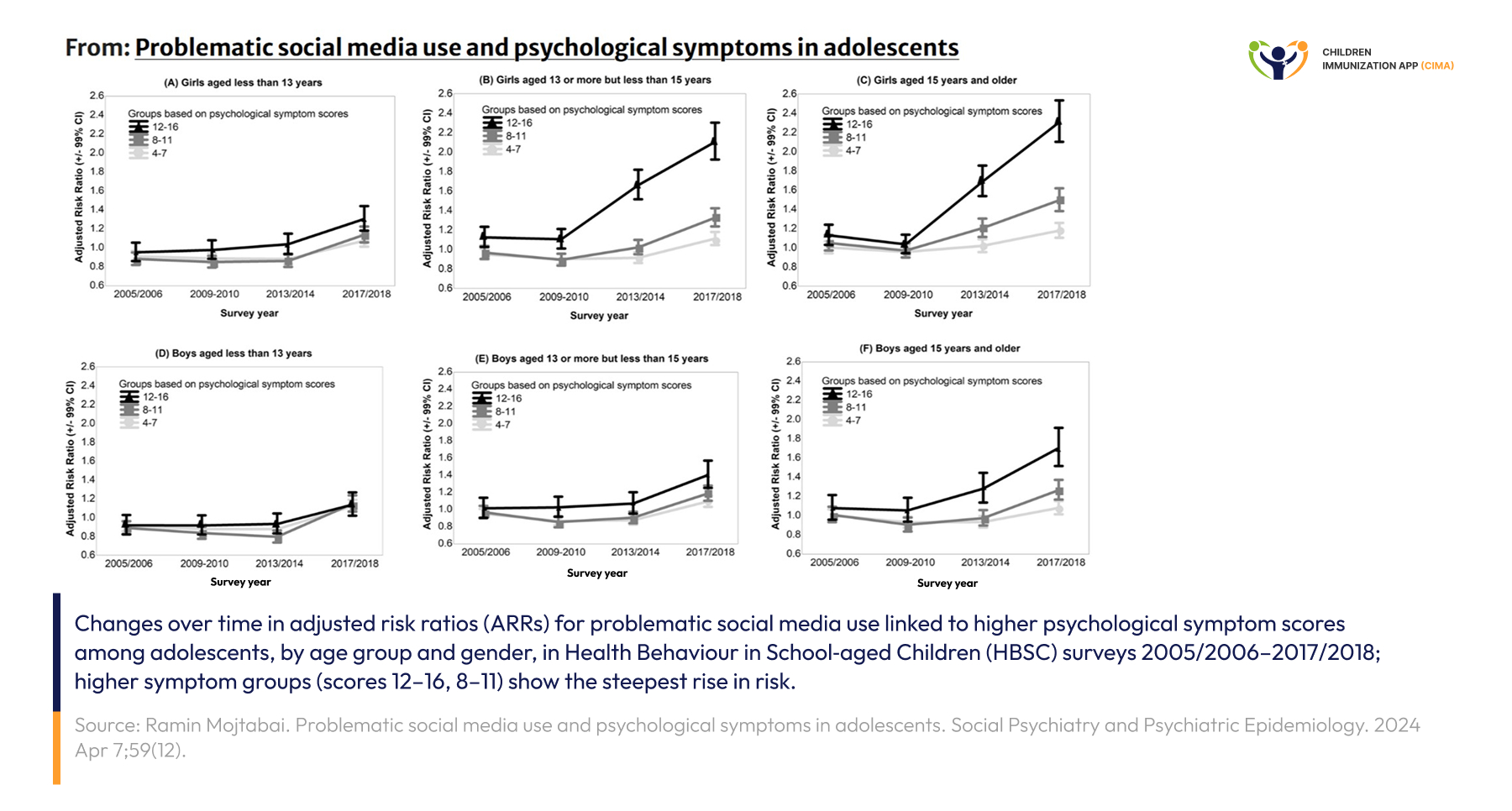
The mental health signal is real — rising ARRs confirm social media's growing risk to adolescents.
2. Artificial Inteligence Enters the Family — and the Conversation Must Catch Up
Dr. Ying Xu, Assistant Professor of AI in Learning and Education at Harvard University, advises in UNICEF's “Parenting in the AI age" that parents can start talking about AI when children are quite young, because many already encounter AI in their everyday lives—through games, voice assistants, recommendation systems, and increasingly through AI chatbots. Her central message is that AI risks are not only about how products are built (privacy, manipulative design, harmful or misleading content), but also about how AI shapes how children learn, solve problems, and form relationships. AI tools that are always agreeable or relentlessly encouraging can create unrealistic expectations of friendship, while over‑reliance on AI to answer questions or finish tasks can erode the “productive struggle" children need for deep learning and critical thinking. [26-29]
Xu describes warning signs of unhealthy AI use in very practical terms: long or intense sessions, distress or anger when asked to stop, secrecy around what children are doing with AI, and AI time crowding out sleep, schoolwork, or in‑person social life. Her recommended response is conversation, not punishment: parents should stay curious, ask children how AI tools work and how they feel when using them, and set shared expectations. As she puts it, families should "pay attention to AI, but keep it in perspective"; what ultimately matters is not the technology itself, but the environment in which children grow, learn, and thrive—and parents remain a central part of that environment.[26-30]
When 'How can I help you?' replaces the productive struggle—Harvard's AI-in-learning warning.
3. Cyberbullying: Permanent, Public, Faceless
Dr. Sameer Hinduja, Co‑Director of the Cyberbullying Research Center, notes that cyberbullying differs from face‑to‑face bullying because it can be widely visible, permanently stored, and sometimes anonymous or "faceless," which can intensify anxiety, shame, and isolation for young people. Research he cites shows that adolescents targeted by cyberbullying report higher levels of depression, anxiety, loneliness, suicidal thoughts or behaviour, and physical symptoms such as pain, fatigue, or shortness of breath.
His advice to parents is equally clear: create a non‑judgmental environment, listen first, document what is happening, and use platform tools like mute, block, and report systematically instead of responding in anger. Above all, he urges adults to validate children's experiences: targets of cyberbullying—and bystanders who witness it—need to know that when they disclose, the adults they tell will respond calmly, rationally, and in ways that make the situation better, not worse. [25 & 31-33]
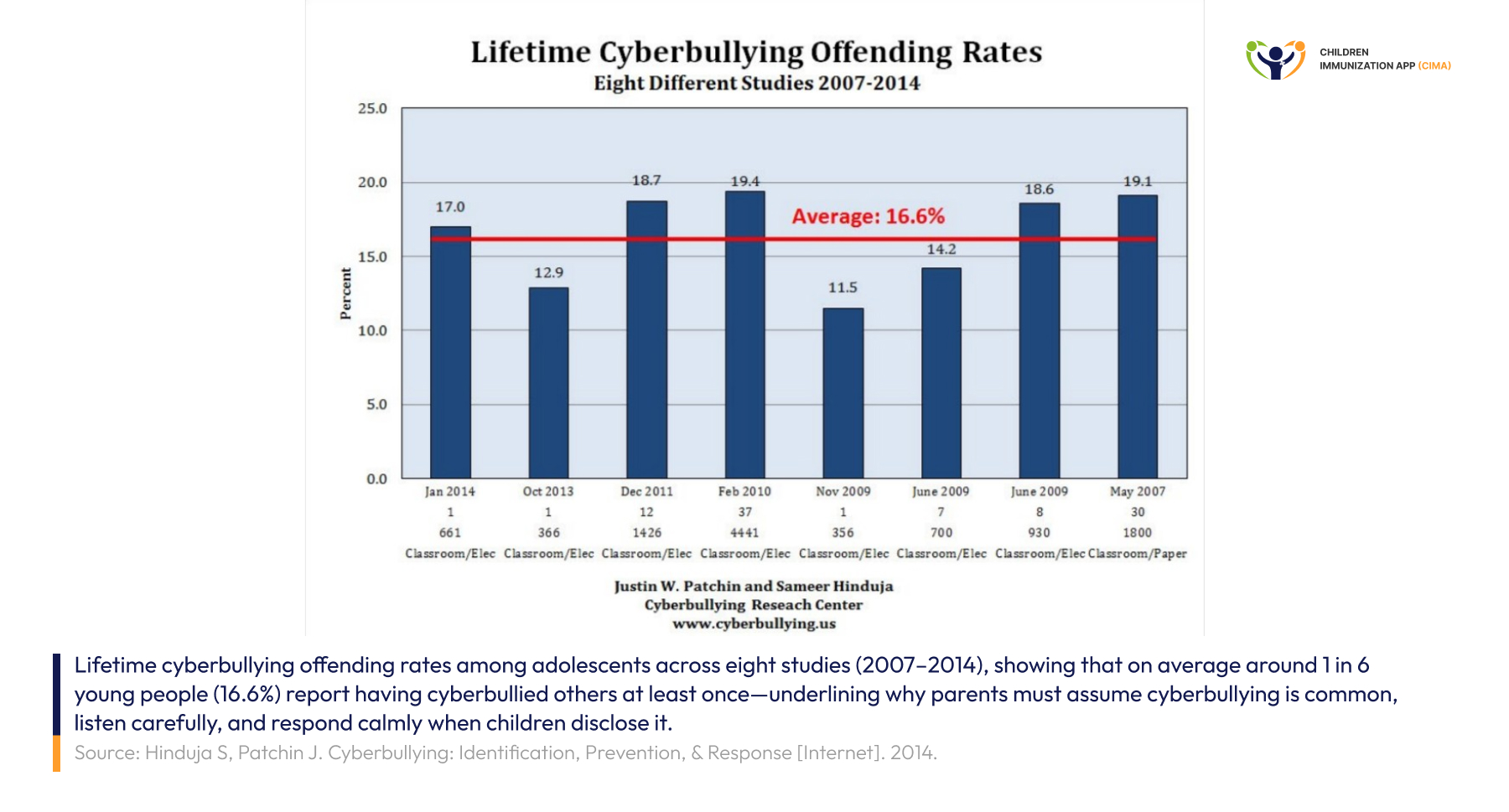
Across 8 studies, 1 in 6 young people has cyberbullied—Dr. Hinduja's data behind the crisis.
Digital Health: Where Children's Rights Begin in Infancy
Long before children own a smartphone, the digital environment is already shaping their right to health. UNICEF is clear that "digitally enabled health systems drive results for children," highlighting benefits such as better quality of care, real‑time data for equity, fewer medical errors, more tailored interventions, and more efficient frontline workers—advantages that matter most where systems are weakest. [34-37]
The evidence base in sub‑Saharan Africa has expanded rapidly. In 2024, only about 54.1% of children in sub‑Saharan Africa were fully vaccinated, far below the WHO global target of 90% coverage by 2030, with the largest gaps in conflict‑affected and remote settings. [38] A 2025 PLOS One systematic review of mHealth and digital health interventions across 19 sub‑Saharan African countries found that tools such as SMS, voice calls, and mobile apps were generally associated with improvements in childhood vaccination coverage and timeliness, with interventions including voice components appearing particularly promising. However, the certainty of evidence ranged from very low to moderate.
A 2025 BMJ Global Health scoping review on demand‑side interventions further noted that while financial incentives can produce short‑term gains, they risk undermining intrinsic motivation and creating dependency, and instead recommended locally acceptable non‑monetary approaches that fit within existing health systems. [18]
Taken together, these findings converge on a clear recommendation: digital health for children must be evidence‑based, integrated, equity‑focused, and built around families rather than one‑off incentives. [18 & 34-38] The philosophy that underpins CIMA Care's model, which uses proven digital tools to support parents, strengthen routine immunization, and advance every child's right to health from infancy onward.
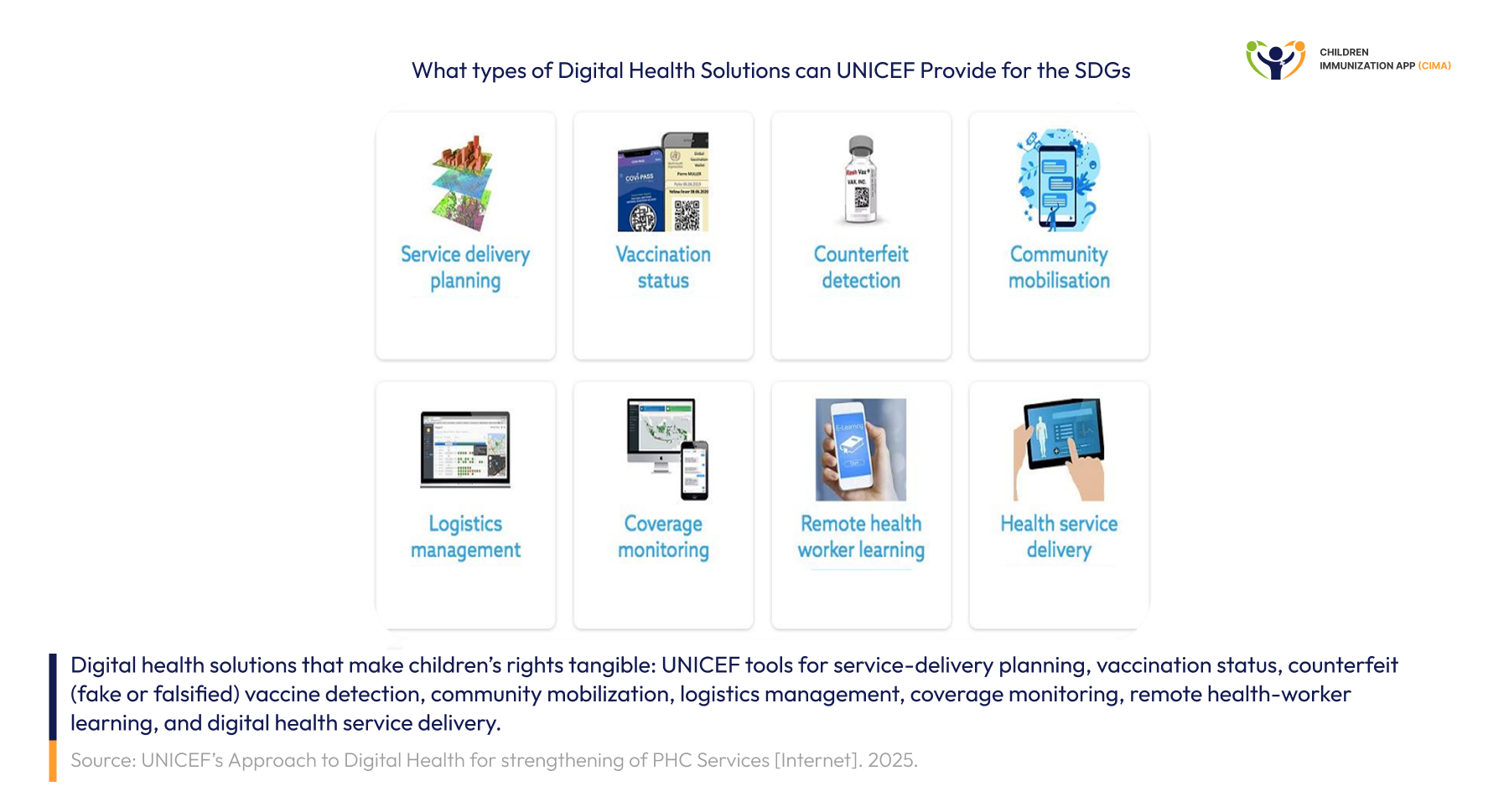
Eight UNICEF digital health tools for children's rights—the ecosystem CIMA Care is built on.
Northwest Cameroon: A Crisis Test for Digital Rights — and a Story of Hope
Few contexts test the promise of digital health more severely than Cameroon's Northwest and Southwest regions. Years of socio‑political crisis have displaced families, closed schools, and created regular “ghost‑town" days that interrupt routine vaccination and other basic services. [39-40]
In these regions, partners report that routine immunization coverage in some conflict‑affected districts has dropped by as much as 60%, leaving large numbers of children under‑ or unvaccinated and vulnerable to vaccine‑preventable diseases. Gavi notes that coverage has fallen below 30% in some areas of the Northwest and Southwest, with an estimated 40% of health facilities non‑functional. [39-41]
Across Cameroon as a whole, the wider humanitarian crisis has driven large‑scale displacement. Recent UNICEF Cameroon situation reports, and humanitarian dashboards estimate that more than 2 million people are now forcibly displaced—including internally displaced persons, refugees, returnees, and asylum‑seekers—with children accounting for over half of those in need of assistance. [40 & 42]
Against this backdrop, CIMA Care's pilot at the Bamenda Regional Hospital and the Azire, Atuakom, and Mulang Integrated Health Centers has become a living demonstration that digital rights can be claimed even when state systems are under strain. Dr. Cornelius Chebo, EPI Coordinator for the Northwest Region of Cameroon, told Star TV:
"If you look at the performance in the health facilities where the CIMA project is being implemented, in fact, we have more than 99% success rates of children that are not missing out on vaccines as compared to the other areas where it is not. … We use all the available opportunities, including the technological and the physical ones, the human aspect of it." [50]
Moreover, Associate Professor George Ikomey Mondinde of the University of Yaoundé 1 affirmed:
"The CIMA project has demonstrated the usefulness of the reminder app in improving vaccine coverage in Cameroon, particularly in the crisis-hit zones of Bamenda in the Northwest region." [6]
Even where literacy is limited, the rights-respecting design carries through. Dr. Chebo explains:
"That is why I said even the health facility receives notification also. Because when the parent cannot read, the health facility now has the opportunity to call." [50] This dual-channel architecture honors the child's right to non-discrimination and the household's right to be heard — features which UNESCO's 2020 Global Education Monitoring Report identifies as essential for inclusion in regions where functional illiteracy among rural women remains high. [52]
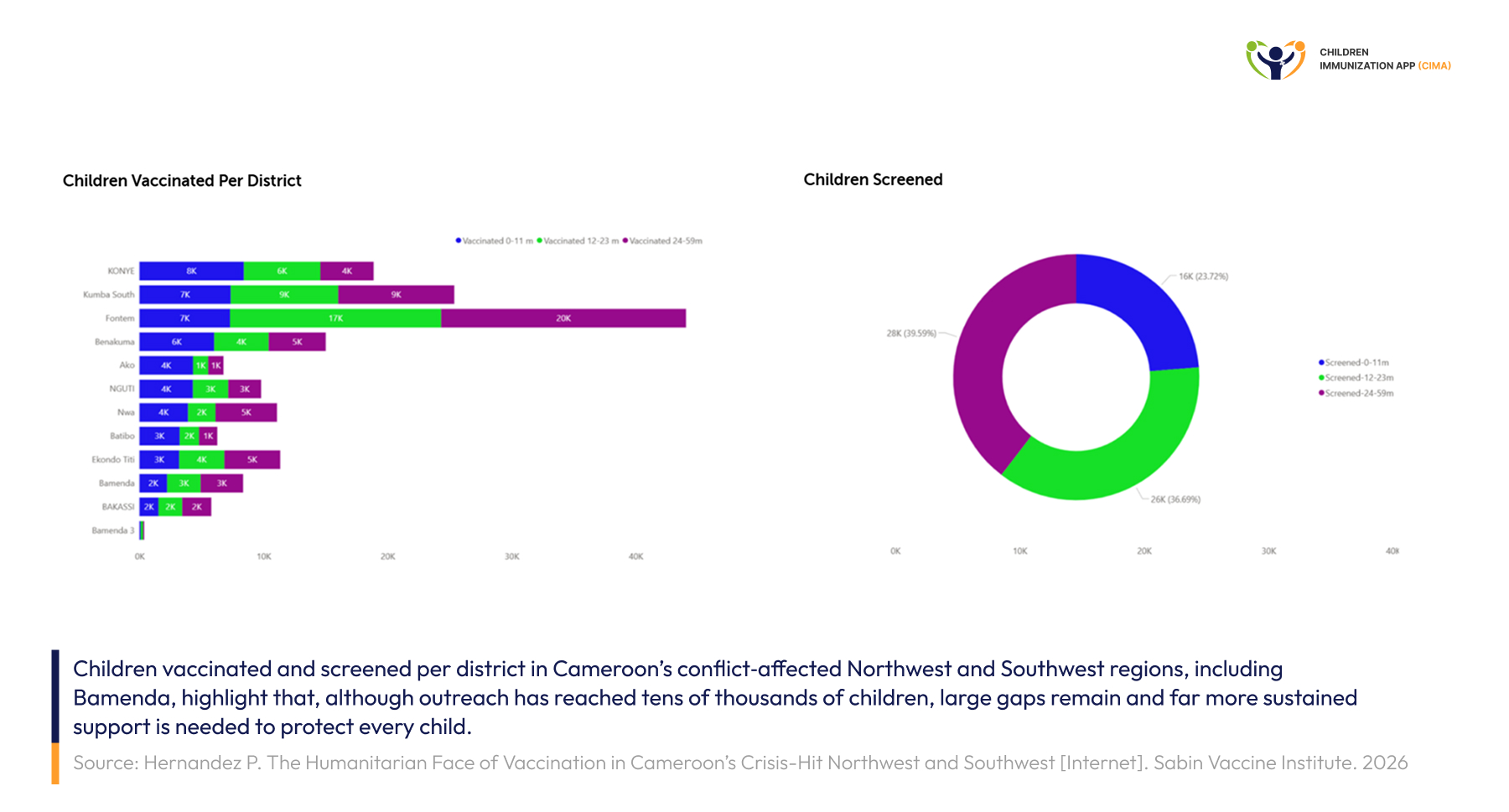
Tens of thousands were reached in crisis-hit Cameroon—yet the gaps demand digital tools.
Beyond Vaccination: How CIMA Care Supports Parents and Households in Northwest Cameroon
Children's rights cannot be honored one at a time. The right to health depends on the rights to information, to family life, and to household support during transitions such as infancy, adolescence, and crisis. CIMA Care's design recognizes this, and it is why UNODC singled out the platform in 2024 in its global report, "A Year of Collective Action for Evidence-Based Drug Use Prevention." [4]
What does this look like for a household in Bamenda?
1.Evidence-Based Parenting Messages, Curated by UNICEF, UNODC, and WHO
Each registered family receives multilingual SMS messages aligned to the child's developmental milestones and vaccination schedule. The content draws from UNODC's parenting skills materials (the same evidence base behind "Family United" and "Friends in Focus"), UNICEF's positive parenting tips, and WHO's child-health guidance. Yayah Emerencia Ngah, PhD student at Texila American University and a CIMA Care field champion, explains on Star TV: "This digital tool is actually more than [reminders]… we have messages on parenting skills and messages on the care of the baby. These messages are actually developed by UNICEF and the United Nations Office on Drugs and Crime (UNDOC)."
The relevance is profound. As Yayah notes for the Northwest Region, where teenage pregnancy is common, "these girls don't actually know how to take care of babies," and a respectful, on-time SMS that arrives in the parents' preferred language can be the difference between fear and confidence. [43]
From fear to confidence—CIMA Care field champion Yayah Ngah explains on Cameroon's Star TV.
2. Reaching the Whole Household — Including Parents Who Cannot Read
CIMA Care turns a missed appointment into a second chance, not a dead end. The app sends parents an early alert before each due date so they can plan transport, arrange care for other children, or request time off work, followed by additional reminders over the next two days if a visit is missed. After every dose, the child’s digital vaccination record is automatically updated in the app, giving caregivers a simple, up‑to‑date history they can understand at a glance. At the same time, nurses and other health workers see scheduled, on‑time, and defaulted doses on the CIMA Care dashboard—complete with a vaccination “heat map” that highlights gaps—so clinics can call families, reach illiterate caregivers by phone, and mobilize community health workers to knock on doors and recover children who might otherwise be left unprotected. In line with UNICEF’s guidance on people‑centered digital health, CIMA Care's three-pillar approach ensures that digital systems work alongside the human relationships that make health services trustworthy, rather than trying to replace them. [17 & 44]

A missed appointment should become a knock on the door, especially for mothers who cannot read—CIMA Care provides different ways to leave no baby unprotected.
3. Supporting Mothers' Mental Wellbeing and Family Bonds
A mother interviewed at the Bamenda Regional Hospital shared on Star TV: "The first time I received the message, I was surprised… So, I'll be surprised, and I'll be happy too… It is very important we take the vaccine." [7] Nurse Fongang Vera Imba at Atuakom adds: "Parents are deeply encouraged and uplifted by the support they receive through CIMA Care's SMS messages, which provide valuable guidance on parenting and child development. Despite facing various challenges, these messages offer reassurance, helping parents stay informed and confident in their parenting journey." [45]
These testimonies map onto a literature signal that is now well established in 2025: community-engaged, dialogue-based digital interventions outperform top-down delivery by building trust and ownership, particularly in fragile contexts. [46]

Surprised and happy 'too'—mothers at Bamenda Regional Hospital testify to CIMA Care's uplift.
4. Empowerment, Not Dependency
Following the 2025 BMJ Global Health scoping review on incentives, which warned that financial rewards can erode "self-determination" and create "payment expectations" that undermine future participation, [47] CIMA Care's empowerment model offers a clear alternative: equip parents with knowledge and reminders rather than payments, equip healthcare workers with CPD-certified training and digital tools rather than ad hoc bonuses, and equip the system itself with real-time data rather than dependent enrollment incentives. [48]
Knowledge for parents, CPD for health workers, data for systems — CIMA Care empowers, not pays only.
From Pilot to Scale: How the Same Model Translates Across Continents
CIMA Care's impact in Bamenda is already measurable and explicitly documented, and Dr. Chebo clearly frames it as a model for wider use. Building on a documented 23% improvement in vaccination uptake in Bamenda, Cameroon, [49] CIMA Care's platform has been endorsed by Dr. Cornelius Chebo, EPI Coordinator for the Northwest Region, who has publicly called for its expansion beyond the Bamenda pilot—underscoring that the design is scalable and not limited to a single district. [50]
But CIMA Care's design is not specific to Bamenda. The same architecture has led to a 19% growth in vaccination uptake in Jordan's Zaatari Refugee Camp, where multilingual outreach is critical. Moreover, CIMA Health Academy has trained over 4,000 healthcare professionals from 77+ countries through its CPD-certified, expanding curriculum on the Arena Learning Management System, awarding 14.42 CPD credits across 31 specialized modules. The academy's strategic partnerships span Jordan CDC's national academic alliance, Cameroon's EPI, Rwanda Biomedical Center, Lebanese American University, Higher Colleges of Technology (HCT-UAE), and the University of Linongwe. [51]
UNICEF Rwanda’s “From piles of registers to digital care” case study shows how a community electronic medical records (cEMR) system, piloted with 600 community health workers (CHWs) in five districts, is now being scaled to reach Rwanda’s full CHW workforce—around 58,567 CHWs nationwide—demonstrating that, with sustained investment and national leadership, digital tools designed for low‑resource settings can help close the service‑delivery gap instead of widening it. [8 & 53-54]
Recent case studies show that when community health workers are supported with digital tools—such as electronic supervision checklists, stock‑tracking dashboards, and mobile reminder systems—they improve defaulter tracing and real‑time vaccine supply management, helping keep immunization services running in hard‑to‑reach areas. [56-57]
CIMA Care's CHW-facing dashboards and CIMA Health Academy's WHO-aligned "Empowering Community Health Champions" course (47:11:00, 3.7 CPD credits) are designed precisely for this — turning the global evidence base into local capability. [51 & 58]

Rwankeri CHWs raise smartphones—proof that digital tools can scale from 600 pilots to 58,567.
What Healthcare Workers Can Do Now — A Rights-Based Checklist
For healthcare professionals, community health workers, parents, and any reader committed to children's digital rights, the practical synthesis of UNICEF, WHO, and recent peer-reviewed evidence is clear:
- Digital policy and practice must start with children’s rights, not from fear. GC25 confirms that States must promote, respect, protect, and fulfill all rights in the digital environment—including children’s rights to health, education, participation, and protection—rather than treating the digital world only as a source of risk. [20]
- Use evidence-based digital reminders. SMS reminders increased childhood immunization coverage and timeliness in low- and middle-income countries (RR 1.16 and 1.21, respectively). [19]
- Adopt voice + SMS for the lowest-literacy contexts. Voice-based components tended to yield larger gains in vaccination coverage and timeliness in the 2025 sub-Saharan systematic review. [18]
- Minimize data, maximize purpose. Apply UNICEF's purpose-specific and minimal data collection principles to every digital health record. [21 & 59]
- Invest in CHWs as digital champions. Equip them with smartphones, training, mentorship, and supportive supervision — as Rwanda's cEMR rollout has demonstrated at the national scale. [8]
- Choose empowerment over financial incentives. Build intrinsic motivation through CPD-certified training and skills, not cash. [47]
- Treat the family as the unit of care. UNICEF's Digital Parenting resources are written for parents and caregivers together, encouraging mothers, fathers, and other caregivers to build healthy digital habits as a family, which is especially important during stressful or crises. [9]
- Use UNICEF tools to talk early and often. Draw on UNICEF's Digital Parenting hub, “Parenting in the AI age,” and its cyberbullying guide to start age‑appropriate conversations about AI, privacy, online safety, and cyberbullying—and to keep those conversations going over time. [9, 21 & 25]
- Document, learn, scale. Real-time monitoring, defaulter tracking, and AEFI surveillance turn digital systems into living evidence engines. [17]

Children's rights first — nine evidence-based actions every health worker can do now.
CIMA Care — Honoring Every Child's Digital Rights, from the First SMS Onward
Children's rights in a digital world are not realized in the abstract. They are realized in the moment a mother in Azire opens an SMS that says, "Your baby is due for a vaccine tomorrow." They are realized when an illiterate caregiver receives a phone call from a nurse who, through the digital platform, knows that her child has not arrived for the vaccination appointment. They are realized when a community health worker receives a list of defaulters and walks to a household in a hard-to-reach village. They are realized when an evidence-based parenting message, validated by UNICEF and UNODC, arrives in a young mother's preferred language on a day she most needs it.
This is the work CIMA Care is doing every day. But CIMA Care is more than an app. It is a child rights instrument: a digital reminder that becomes a protected child; a CPD-certified course that becomes a confident healthcare worker; a parenting tip that becomes a stronger family bond; a heat map that becomes equitable resource allocation; a defaulter list that becomes a knock on the door.
CIMA Care is committed to building a healthier, more equitable digital future — one household at a time, beginning with the youngest child.
If you are a parent, a healthcare worker, a community health worker, a researcher, an academic institution, a Ministry of Health, an NGO, or a private-sector partner, your role in the digital protection of children matters, and there is a place for you in this work.

'Your baby is due for a vaccine tomorrow.' — the SMS that becomes a protected child.
Turn Digital Tools Into Rights Realized — Connect With CIMA Care
Visit www.cima.care to discover how our integrated parenting-vaccination and academic ecosystem can strengthen children's rights in your community. Whether you want to enroll in a CPD-certified course, partner on implementation, or bring CIMA Care's proven model to your country, we are ready to walk that road with you.
Email support@cima.care
or
Write to us at https://www.cima.care/contact
And let us protect every child's digital rights.

One nurse, one child, one bandage—join CIMA Care and turn digital tools into rights realized.
Image References
- 1. United Nations Children’s Fund (UNICEF). The State of the World’s Children 2025: Ending child poverty: Our shared imperative [Internet]. New York: UNICEF; 2025 [cited 2026 May 26]. Available from: https://www.unicef.org/reports/state-of-worlds-children/2025#download
- 2. Author(s) unknown. Article available on PubMed Central [Internet]. PubMed Central; [cited 2026 May 26]. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10050023/
- 3. CIMA Care. Stories [Internet]. CIMA Care; [cited 2026 May 26]. Available from: https://www.cima.care/insights/stories/
Blog Resources
- 1- United Nations. OHCHR | General comment No. 25 (2021) on children's rights in relation to the digital environment [Internet]. OHCHR. 2021. Available from: https://www.ohchr.org/en/documents/general-comments-and-recommendations/general-comment-no-25-2021-childrens-rights-relation2- Committee on the Rights of the Child General comment No. 25 (2021) on children's rights in relation to the digital environment | Better Care Network [Internet]. Bettercarenetwork.org. 2021 [cited 2026 May 3]. Available from: https://bettercarenetwork.org/library/social-welfare-systems/child-care-and-protection-policies/committee-on-the-rights-of-the-child-general-comment-no-25-2021-on-children%E2%80%99s-rights-in-relation-to3- Children want to shape their rights in the digital world [Internet]. OHCHR. 2025. Available from: https://www.ohchr.org/en/stories/2025/11/children-want-shape-their-rights-digital-world4- A Year of Collective Action for Evidence-Based Drug Use Prevention [Internet]. United Nations: Office on Drugs and Crime. 2021. Available from: https://www.unodc.org/unodc/drug-prevention-and-treatment/news-and-events/2025/january/a-year-of-collective-action-for-evidence-based-drug-use-prevention.html5- UNODC Recognizes CIMA Care's Digital Health Innovation [Internet]. Cima.care. 2025 [cited 2026 May 3]. Available from: https://www.cima.care/insights/unodc-recognized-digital-technology-child-health/6- Digital Innovation Meets Mother's Love: CIMA's Revolution in Child Health [Internet]. Cima.care. 2024 [cited 2026 May 3]. Available from: https://www.cima.care/insights/fr/cima-mothers-child-health-innovation/7- When Caregivers Remember: Mothers’ Voices Reveal CIMA Care's Heartfelt Impact at Bamenda Regional Hospital [Internet]. Cima.care. 2025 [cited 2026 May 3]. Available from: https://www.cima.care/insights/cima-care-mothers-voices-bamenda-hospital/8- Iyakaremye T. From Piles of Registers to Digital Care: Community Health Workers in Rwanda Adopt Digital Health Rec [Internet]. Unicef.org. 2016. Available from: https://www.unicef.org/rwanda/stories/piles-registers-digital-care-community-health-workers-rwanda-adopt-digital-health-rec9- Digital parenting [Internet]. Unicef.org. 2024. Available from: https://www.unicef.org/parenting/digital-parenting10- Digitalization [Internet]. unicef.ch. 2021 [cited 2026 May 3]. Available from: https://www.unicef.ch/en/what-we-do/national/digitalization11- Reshaping the digital world for Aussie kids [Internet]. Available from: https://assets-us-01.kc-usercontent.com/99f113b4-e5f7-00d2-23c0-c83ca2e4cfa2/6cde226b-23d1-413a-bac3-7f0eafe524d4/UA_Digital-Wellbeing-Position-Paper-2024_LR_FINAL.pdf12- Özkul D, Vosloo S, Baghdasaryan B. Best Interests of the Child in Relation to the Digital Environment [Internet]. 2025. Available from: https://www.unicef.org/innocenti/media/10571/file/UNICEF-Innocenti-Best-interests-child-digital-environment-brief-2025.pdf13- Age restrictions alone won’t keep children safe online [Internet]. Unicef.org. 2025. Available from: https://www.unicef.org/press-releases/age-restrictions-alone-wont-keep-children-safe-online14- Children's rights in the digital sphere – promotion of media literacy instead of bans [Internet]. unicef.ch. 2024. Available from: https://www.unicef.ch/en/current/news/2024-12-13/children-s-rights-digital-sphere-promotion-media-literacy-instead-bans15- UNICEF. The State of the World’s Children 2024 [Internet]. Unicef.org. 2024. Available from: https://www.unicef.org/reports/state-of-worlds-children/202416- HOW MANY CHILDREN AND YOUNG PEOPLE HAVE INTERNET ACCESS AT HOME? [Internet]. Available from: https://www.unicef.or.jp/jcu-cms/media-contents/2020/12/How_many_children_Young_ppl_have_access_to_internet_final_v2.pdf17- Digital health [Internet]. Unicef.org. 2024. Available from: https://www.unicef.org/digitalimpact/what-we-do/digital-health18- Bhattacharya A, Mark-Uchendu C, Hansen C, Evans J. Systematic review of mHealth and digital health interventions to improve childhood vaccination uptake in 19 Sub-Saharan African countries. Umer MF, editor. PLOS One [Internet]. 2025 Dec 23 [cited 2026 Feb 21];20(12):e0324117. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12725567/20- Welcome To Zscaler Directory Authentication [Internet]. Unicef.org. 2026. Available from: https://www.unicef.org/bulgaria/en/media/10596/file21- Xu Y. Parenting in the AI age [Internet]. UNICEF; 2026 [cited 2026 May 3]. Available from: https://www.unicef.org/parenting/digital-parenting/how-approach-ai-children22- World Health Organization. Teens, screens, and mental health [Internet]. World Health Organization. World Health Organization; 2024. Available from: https://www.who.int/europe/news/item/25-09-2024-teens--screens-and-mental-health23- World Health Organization Regional Office for Europe. 11% of teens struggle with problematic social media use: child and adolescent health in Europe [Internet]. Copenhagen: WHO Regional Office for Europe; 2024 [cited 2026 May 4]. Available from: https://iris.who.int/server/api/core/bitstreams/30bc5231-b9de-45fa-9e25-eb329c23689f/content25- Hinduja S. How to talk to your child about cyberbullying [Internet]. Unicef.org. 2025. Available from: https://www.unicef.org/parenting/child-care/what-to-do-if-your-child-is-experiencing-cyberbullying26- 4.6K reactions · 43 shares | From homework help to smart devices, AI is becoming a part of life for many families. Understanding both the benefits and risks helps parents guide their children with confidence. | UNICEF [Internet]. Facebook.com. 2016 [cited 2026 May 4]. Available from: https://www.facebook.com/unicef/videos/parenting-in-the-ai-age-unicef-parenting/799061312486616/27- Anderson J. The Impact of AI on Children’s Development [Internet]. Harvard Graduate School of Education. EdCast; 2024. Available from: https://www.gse.harvard.edu/ideas/edcast/24/10/impact-ai-childrens-development28- Children and Screens. AI’s Impact on Children’s Social and Cognitive Development with Ying Xu, PhD [Internet]. YouTube. 2025. Available from: https://www.youtube.com/watch?v=YqyPueTOf5g29- Why Education Research Matters: AI and Children [Internet]. Harvard Graduate School of Education. 2025. Available from: https://www.gse.harvard.edu/ideas/news/25/12/why-education-research-matters-ai-and-children30- Pacific U. When children interact with AI, they may see misleading content or reveal sensitive information. [Internet]. LinkedIn. 2026 [cited 2026 May 4]. Available from: https://www.linkedin.com/posts/unicefpacific_parenting-in-the-ai-age-activity-7429353471025516544-HvMB31- Parenting: Protecting Your Child From Cyberbullying | UNICEF USA [Internet]. www.unicefusa.org. Available from: https://www.unicefusa.org/what-unicef-does/parenting/protect-children-cyberbullying32- Preventing cyberbullying: Q&A with Sameer Hinduja – JPRC [Internet]. Wested.org. 2024. Available from: https://jprc.wested.org/preventing-cyberbullying-qa-with-sameer-hinduja/33- Hinduja S, Patchin J. Cyberbullying: Identification, Prevention, & Response [Internet]. 2014. Available from: https://cyberbullying.org/Cyberbullying-Identification-Prevention-Response.pdf35- Digital health [Internet]. Unicef.org. 2024. Available from: https://www.unicef.org/digitalimpact/what-we-do/digital-health36- Contreras A. UNICEF Digital Health approach - WHO Collaborating Centre on Primary Health Care [Internet]. WHO Collaborating Centre on Primary Health Care - WHO Collaborating Centre on Primary Health Care. 2024 [cited 2026 May 4]. Available from: https://primaryhealthcare4people.org/toolkits/unicef-digital-health-approach/37- UNICEF's Approach to Digital Health for strengthening of PHC Services [Internet]. 2025 [cited 2026 May 4]. Available from: https://phd.spc.int/sites/default/files/p-related-files/2025-03/Item%2016.1_PHIN_PPT_UNICEF%20Digital%20Health%20for%20Community%20PHC.pdf38- BMJ Global Health | BMJ Global Health covers all aspects of global health with particular interest in the underfunded area of non-communicable diseases (NCDs). [Internet]. BMJ Global Health. 2019. Available from: https://gh.bmj.com/39- Hernandez P. The Humanitarian Face of Vaccination in Cameroon's Crisis-Hit Northwest and Southwest [Internet]. Sabin Vaccine Institute. 2026 [cited 2026 May 4]. Available from: https://www.sabin.org/resources/the-humanitarian-face-of-vaccination-in-cameroons-crisis-hit-northwest-and-southwest/40- Reaching every child: life-saving vaccines for conflict-affected communities in Cameroon [Internet]. Unicef.org. 2025 [cited 2026 May 4]. Available from: https://www.unicef.org/cameroon/stories/reaching-every-child-life-saving-vaccines-conflict-affected-communities-cameroon41- How a Gavi-supported project is changing lives in conflict-affected Cameroon [Internet]. Gavi.org. 2025. Available from: https://www.gavi.org/vaccineswork/how-gavi-supported-project-changing-lives-conflict-affected-cameroon42- Zero-Dose Children and Vaccine Gaps in Cameroon | Think Global Health [Internet]. Think Global Health. 2024. Available from: https://www.thinkglobalhealth.org/article/zero-dose-children-and-vaccine-gaps-in-cameroon43- From Crisis to Hope: CIMA Care’s Live Television Breakthrough in Northwest Cameroon [Internet]. Cima.care. 2025 [cited 2026 May 4]. Available from: https://www.cima.care/insights/cima-care-live-tv-breakthrough-northwest-cameroon/44- CHILDREN IMMUNIZATION APP (CIMA) Strengthening Global Immunization Systems Through Digital Innovation and Evidence-Based Capacity Building [Internet]. [cited 2026 May 4]. Available from: https://www.cima.care/CIMA-Care-Policy-Brief.pdf45- Digital Innovation Transforms Rural Healthcare: CIMA’s Journey at Atuakom [Internet]. Cima.care. 2025 [cited 2026 May 4]. Available from: https://www.cima.care/insights/cima-digital-innovation-rural-healthcare-atuakom/46- 2025-2026 DIGITAL C O M M U N I T Y E N G A G E M E N T STRATEGY [Internet]. 2025. Available from: https://www.poliokit.org/sites/default/files/2024-12/Digital%20Community%20Engagement%20Strategy%202025-2026%20v.F%2011%20Dec%202024_rev.pdf47- Saunders MJ, Pereboom M, Alvarez JL, Sherlock M, Kartini Gadroen. Incentives in immunisation campaigns in low- and middle-income countries: a scoping review mapping evidence on effectiveness and unintended consequences. BMJ Global Health [Internet]. 2025 Jun 1;10(6):e019662–2. Available from: https://gh.bmj.com/content/10/6/e01966248- CIMA Care’s Empowerment Approach in Northwest Cameroon Addresses Financial Incentive Research Concerns [Internet]. Cima.care. 2025 [cited 2026 May 4]. Available from: https://www.cima.care/insights/beyond-financial-incentives-cima-care-sustainable-health-cameroon/49- Yayah Emerencia Ngah, George Ikomey Mondinde, Rasa Nikooifard, Cornelius Chebo, Shalom Tchokfe Ndoula, Ujjwal Neogi, Claudia Hanson, Tobias Alfven, Eresso Aga, Wadih Mallouf, Ziad El-Khatib; Enhancing vaccination uptake and parenting education through automated SMS service: A non-RCT pilot study in Bamenda, Cameroon; Mediterranean Life Sciences Union Annual Meeting (MedLIFE-24), Istanbul, Türkiye, December 2024.50- From Forgotten to Protected: The Regional Coordinator’s Tes [Internet]. Cima.care. 2025 [cited 2026 May 5]. Available from: https://www.cima.care/insights/protected-cima-care-breakthrough/51- CIMA Health Academ [Internet]. [cited 2026 May 5]. Available from: https://www.cima.care/CIMA-Health-Ctg.pdf52- 2020 - Inclusion and education: all means all [Internet]. Unesco.org. 2020. Available from: https://www.unesco.org/gem-report/en/publication/2020-inclusion-and-education-all-means-all53- Community Health workers Policy undergoes reform for better service delivery [Internet]. Moh.gov.rw. 2022. Available from: https://www.moh.gov.rw/news-detail/community-health-workers-policy-undergoes-reform-for-better-service-delivery54- Checking your browser - reCAPTCHA [Internet]. Nih.gov. 2024 [cited 2026 May 5]. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12673562/#SF255- A Guide to CHW Training and Program Best Practices [Internet]. Cima.care. 2025 [cited 2026 May 5]. Available from: https://www.cima.care/insights/strengthening-chw-programs-sustainability/56- A Guide to CHW Training and Program Best Practices [Internet]. Cima.care. 2025 [cited 2026 May 5]. Available from: https://www.cima.care/insights/strengthening-chw-programs-sustainability/57- Nutley T, Chaney S, Mechael P. Digital Health Interventions for Supportive Supervision of Health Workers Providing Immunisation Services [Internet]. 2024. Available from: https://static1.squarespace.com/static/681ce14a0fa874212985c01b/t/6877fd2d69d28e76453b0583/1752694062140/Technical-Brief-Supportive-Supervision-of-Health-Workers-ENG.pdf58- CIMA Care: Transforming Global Health Through Digital Innovation, Evidence-Based Education, and Unwavering Commitment C H I L D R E N IMMUNIZATION APP (CIMA) [Internet]. [cited 2026 May 5]. Available from: https://www.cima.care/CIMA-Care-Ctg.pdf59- Online privacy checklist for parents | UNICEF Parenting [Internet]. www.unicef.org. Available from: https://www.unicef.org/parenting/child-care/online-privacy
Enjoyed this article?
Share it with your friends on LinkedIn: Children's Rights in a Digital World: Evidence-Based Innovation for Babies, Parents, and Communities—from Northwest Cameroon to the Global Stage ![]()
Follow us on LinkedIn for more updates and insights: Cima Care GmbH ![]()