Revolutionary HPV Vaccination Breakthroughs: Single-Dose Protection, Gender-Neutral Strategies, and the Path to Cervical Cancer Elimination |
March 09, 2026 . 4 Minutes read
HPV Vaccination Evidence: Single-Dose Efficacy, Proven Safety, Optimal Timing, and Insights to Address Vaccine Hesitancy
As the global health community celebrates nearly two decades since the first HPV vaccine approval in 2006, a revolution is quietly transforming cervical cancer prevention. Recent evidence from 2024-2025 is fundamentally reshaping our understanding of HPV vaccination, from dosing schedules and target populations to safety profiles and implementation strategies. [1 & 2]
A Transformative Moment in Cancer Prevention
While cervical cancer remains the fourth most common cancer in women worldwide, causing over 340,000 deaths annually, breakthrough research is revealing that we now possess the tools to eliminate this preventable disease within our lifetime. This article examines the most recent scientific discoveries in HPV vaccination, from single-dose efficacy data that are revolutionizing vaccine accessibility to gender-neutral vaccination strategies that are accelerating global cancer elimination.
For healthcare professionals and public health advocates, understanding these developments is crucial to implementing evidence-based strategies that can save millions of lives and reshape cancer prevention for future generations. [3]

One confident shot, a lifetime protected. HPV vaccination is rewriting cancer's future.
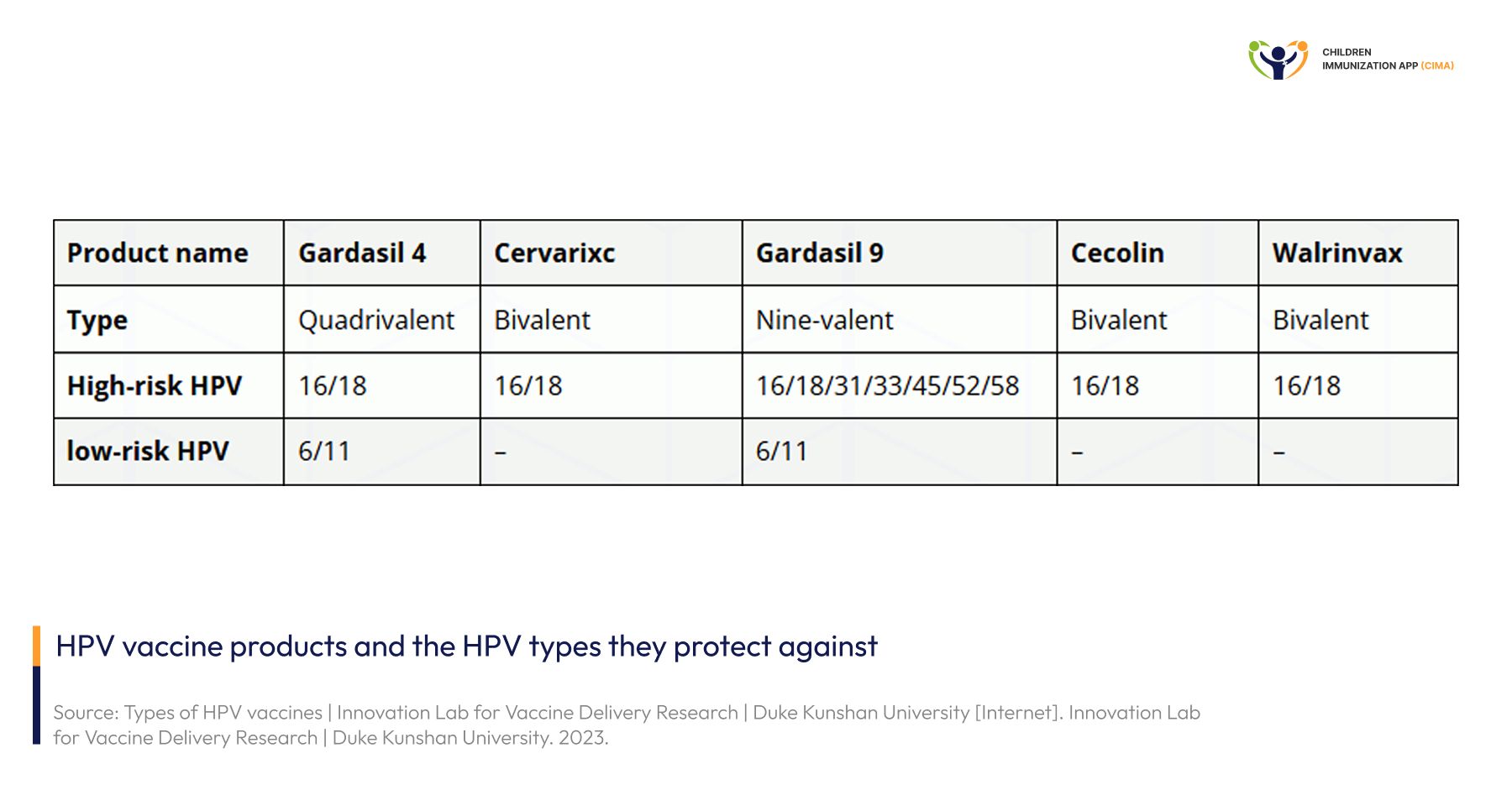
From bivalent to nine-valent: 5 HPV vaccines ranked by strain coverage and protection scope.
Types of HPV and Available Vaccines
Human papillomavirus includes many genotypes, but a small group of high‑risk types (especially HPV16 and 18, and to a lesser extent 31, 33, 45, 52, and 58) cause most HPV‑related cancers, while low‑risk types 6 and 11 mainly cause genital warts. Bivalent vaccines protect against the two key cancer‑causing types, 16 and 18; quadrivalent vaccines add protection against types 6 and 11, preventing most genital warts as well as cervical lesions; and nonavalent vaccines further include types 31, 33, 45, 52, and 58, covering about 90% of cervical cancers and many other anogenital and oropharyngeal cancers. [35 & 36]
The Game-Changing Evidence: Single-Dose HPV Vaccination Achieves 97.5% Efficacy
- 1. Landmark KEN SHE Trial Results Redefine Vaccination Standards
The Kenya Single-dose HPV Efficacy (KEN SHE) trial has delivered some of the most compelling evidence to date that single-dose HPV vaccination provides powerful, sustained protection. Published with extended follow-up data through December 2023, this randomized controlled trial demonstrated that a single dose of HPV vaccine was 97.5% effective in preventing persistent infection with cancer-causing HPV types 16 and 18 among young women aged 15-20 years. [4]
The 3-year durability data, published in Nature Medicine in December 2023, confirmed that single-dose protection remains robust over time, with no evidence of waning efficacy. This finding represents a paradigm shift for global vaccination programs, particularly in low- and middle-income countries where logistical and financial barriers have limited multi-dose coverage. [5]
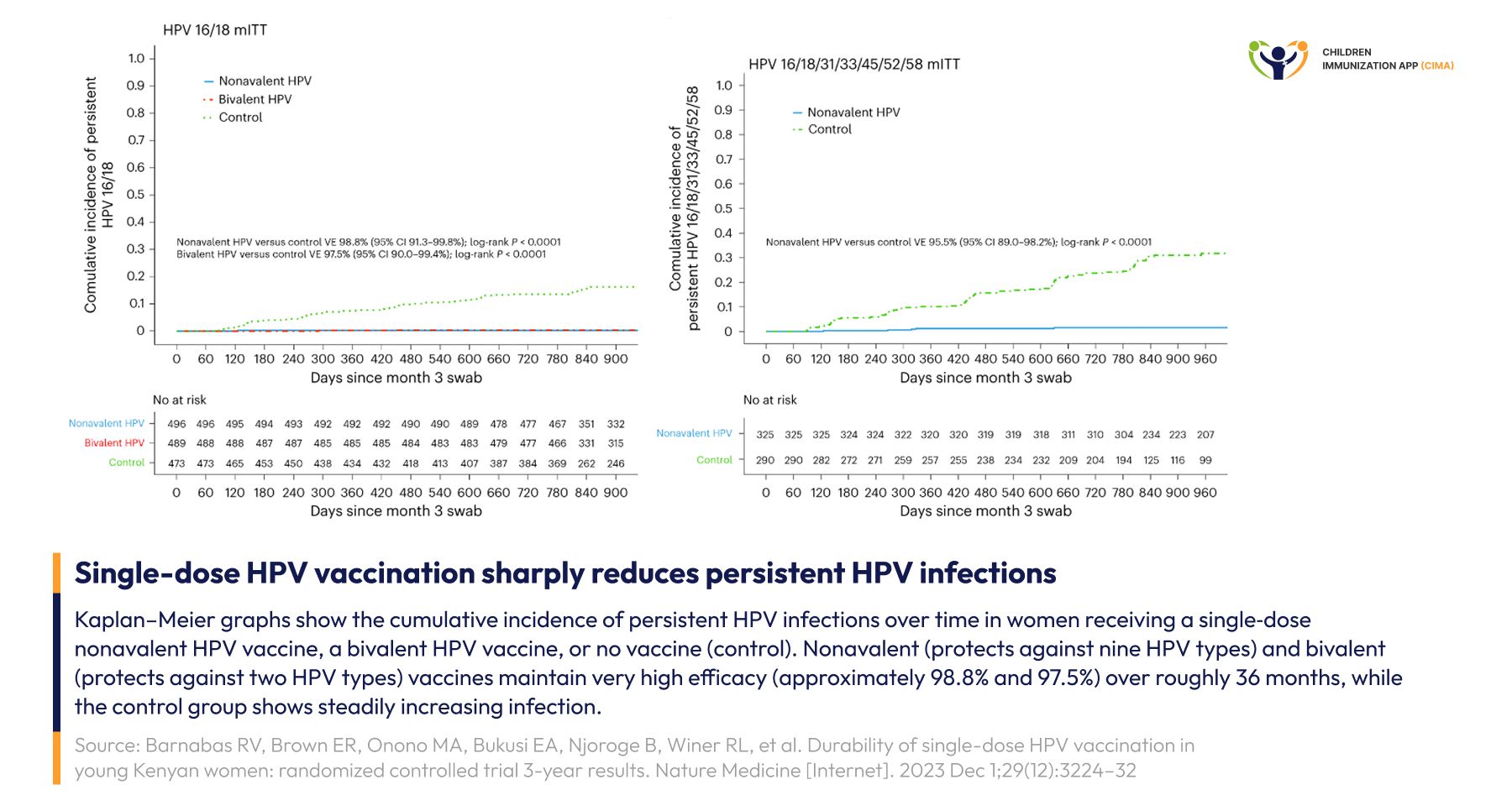
KEN SHE trial: one HPV dose sustains 97.5% efficacy with flat infection curves over 36 months.
2. Immunobridging Evidence from Tanzania Confirms Protection Across Age Groups
The DoRIS (Dose Reduction Immunobridging and Safety Study) trial in Tanzania provided critical evidence that girls aged 9-14 years, the primary target population for HPV vaccination, have peak immune responses comparable to those observed in young women for whom efficacy has been demonstrated. Published in The Lancet Global Health in March 2024, this immunobridging analysis showed that antibody responses 24 months after a single dose were non-inferior to those in the KEN SHE trial participants.[6]
The key difference between KEN SHE and DoRIStrials is who they enrolled and what they measured:
- KEN SHE trial: Randomized efficacy trial in sexually active Kenyan adolescent girls and young women (15–20 years), designed to show that a single HPV vaccine dose prevents new persistent HPV infections (direct clinical protection).
- DoRIS trial: Randomized dose‑reduction and immunobridging trial in Tanzanian girls aged 9–14 years, designed to compare antibody responses (immunogenicity and safety) after one, two, or three doses, and then bridge those antibody levels to efficacy data from trials like KEN SHE and others. [5 & 6]
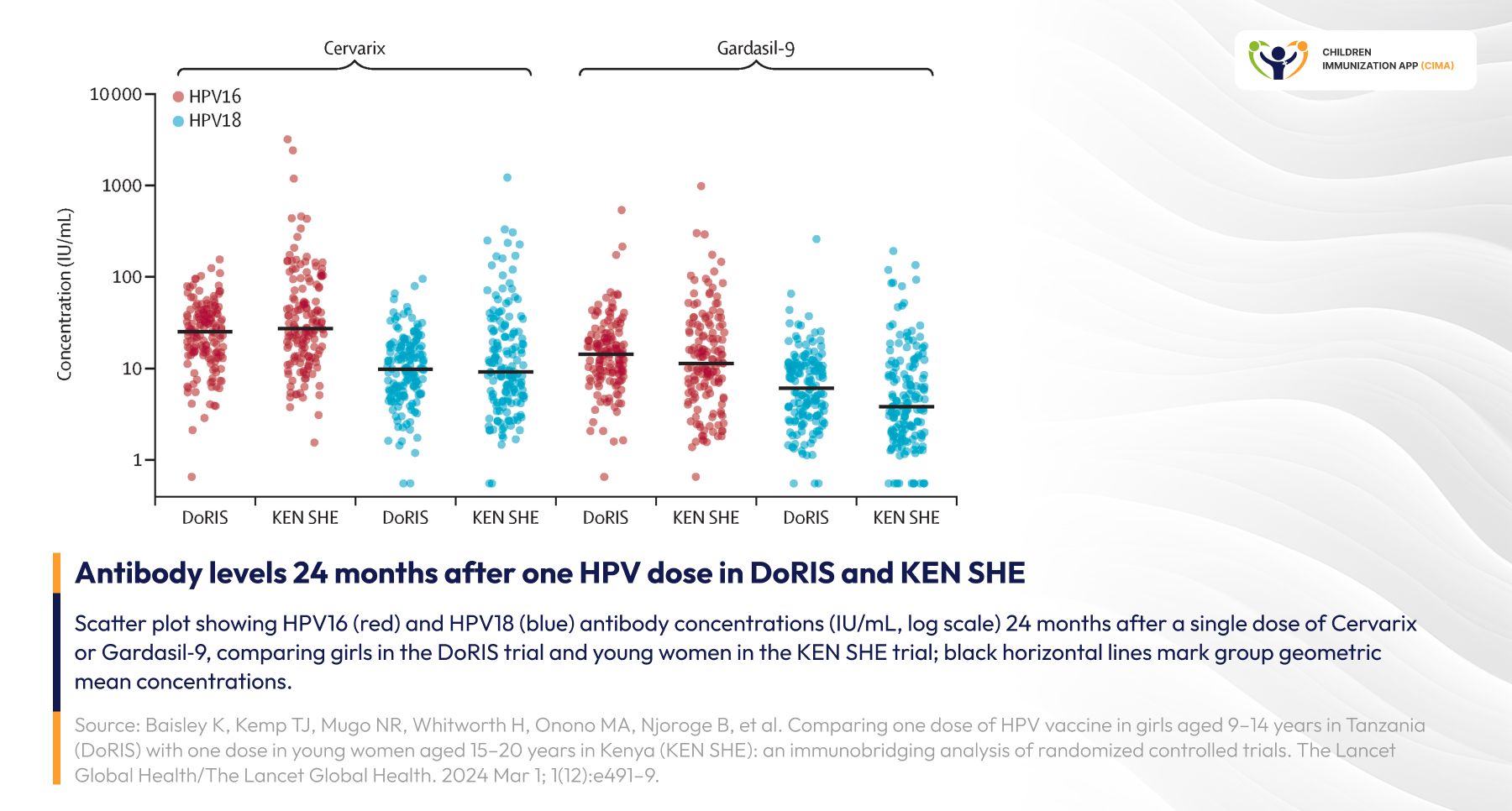
DoRIS trial girls aged 9–14 match KEN SHE women's HPV antibody levels—protection at all ages.
3. Long-Term Durability: 16-Year Follow-Up Shows Sustained Protection
The Costa Rica Vaccine Trial (CVT) continues to provide invaluable long-term data on single-dose protection. In a November 2024 JNCI Monograph publication, researchers reported that HPV16/18 antibody levels remained stably robust 16 years after a single dose of the bivalent HPV vaccine. Researchers found the drop in antibody concentration between years 11 and 16 as "modest" or “small declines”. These stable and robust antibody levels imply women should have protection for at least 20 years and likely much longer, based on the observed patterns of antibody change over time. [7]
Similarly, long‑term follow‑up from the International Agency for Research on Cancer (IARC) India HPV trial shows that a single dose of the quadrivalent (four‑type) HPV vaccine protects girls and young women against both persistent HPV infection and high‑grade cervical precancerous lesions (cervical intraepithelial neoplasia grade 2 or worse, CIN2+) for about 12 years after vaccination. Protection was similarly strong in women who received one, two, or three doses, indicating no added clinical benefit from additional doses. This is the first trial to demonstrate that a single HPV vaccine dose can prevent cervical precancers themselves and not just HPV infection. [8]
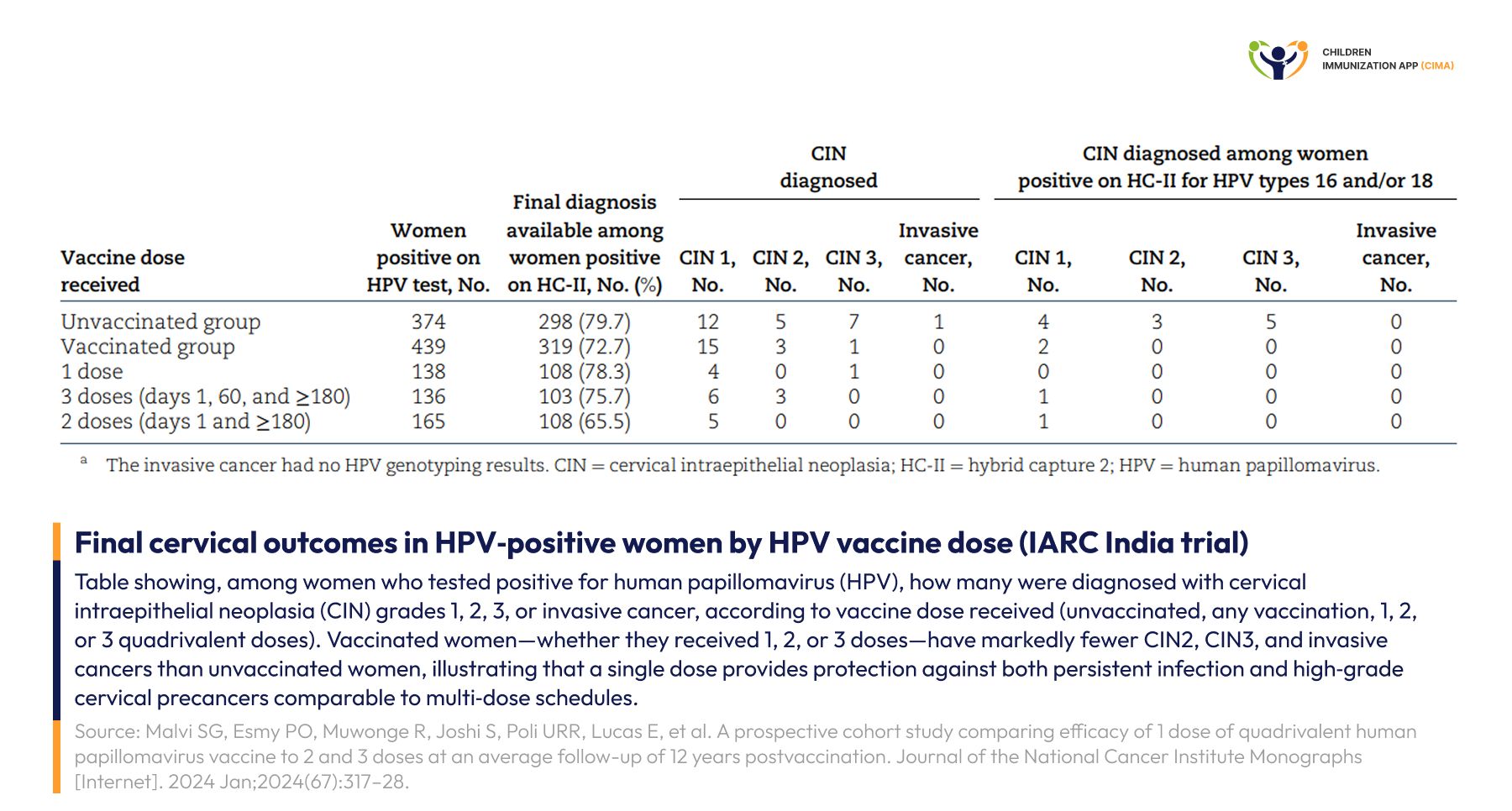
IARC India trial: one HPV dose prevents precancers as effectively as 2 or 3 doses over 12 years.
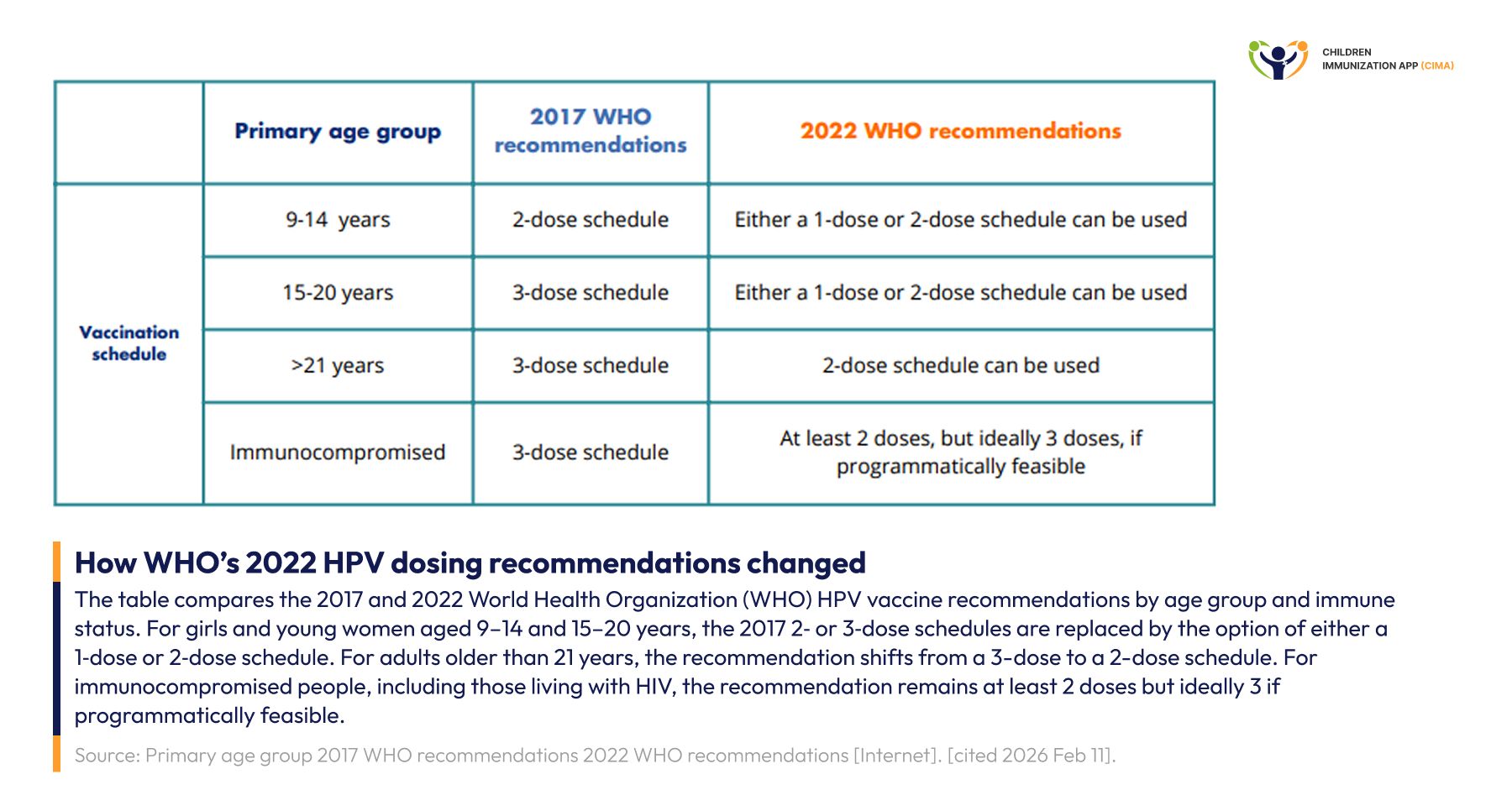
WHO's Bold Recommendation: The Global Shift to Single-Dose Schedules
- 1. Updated 2022 Guidelines Transform Vaccination Strategy
In December 2022, the World Health Organization published a landmark position paper updating HPV vaccine dosing recommendations to include a single-dose schedule as an alternative option for girls and boys aged 9-20 years. This recommendation, based on mounting evidence from KEN SHE, DORIS, CVT, and other studies, states that "a single-dose schedule can provide comparable efficacy and durability of protection as two doses.” [9]
The updated WHO guidance specifies:
- One or two doses: For immunocompetent individuals aged 9-20 years
- Two doses: With a 6-month interval, for those aged 21 years or older
- Three doses: And if not, at least two doses for immunocompromised individuals, including those living with HIV
This policy shift has profound implications for global vaccination programs, potentially doubling or tripling the number of people who can be protected with existing vaccine supplies. [10]
WHO 2022 landmark shift: a single dose is now an option for ages 9–20, doubling global vaccine reach.
2. Real-World Implementation: Countries Embracing Single-Dose
Nigeria became the first African country to introduce HPV vaccination with a single-dose regimen in October 2023,[11] followed by Tanzania in 2024. [12] Kenya officially shifted to single-dose schedules in 2025 for 10-14-year-old girls, with health officials emphasizing that "data has shown that a single dose in girls below 15 years produces a very strong immune response. [13] In September 2023, the United Kingdom introduced a single-dose HPV vaccination offered in school year 8 (12 -13 years old), becoming one of the first high-income countries to adopt this approach as standard practice. [14]
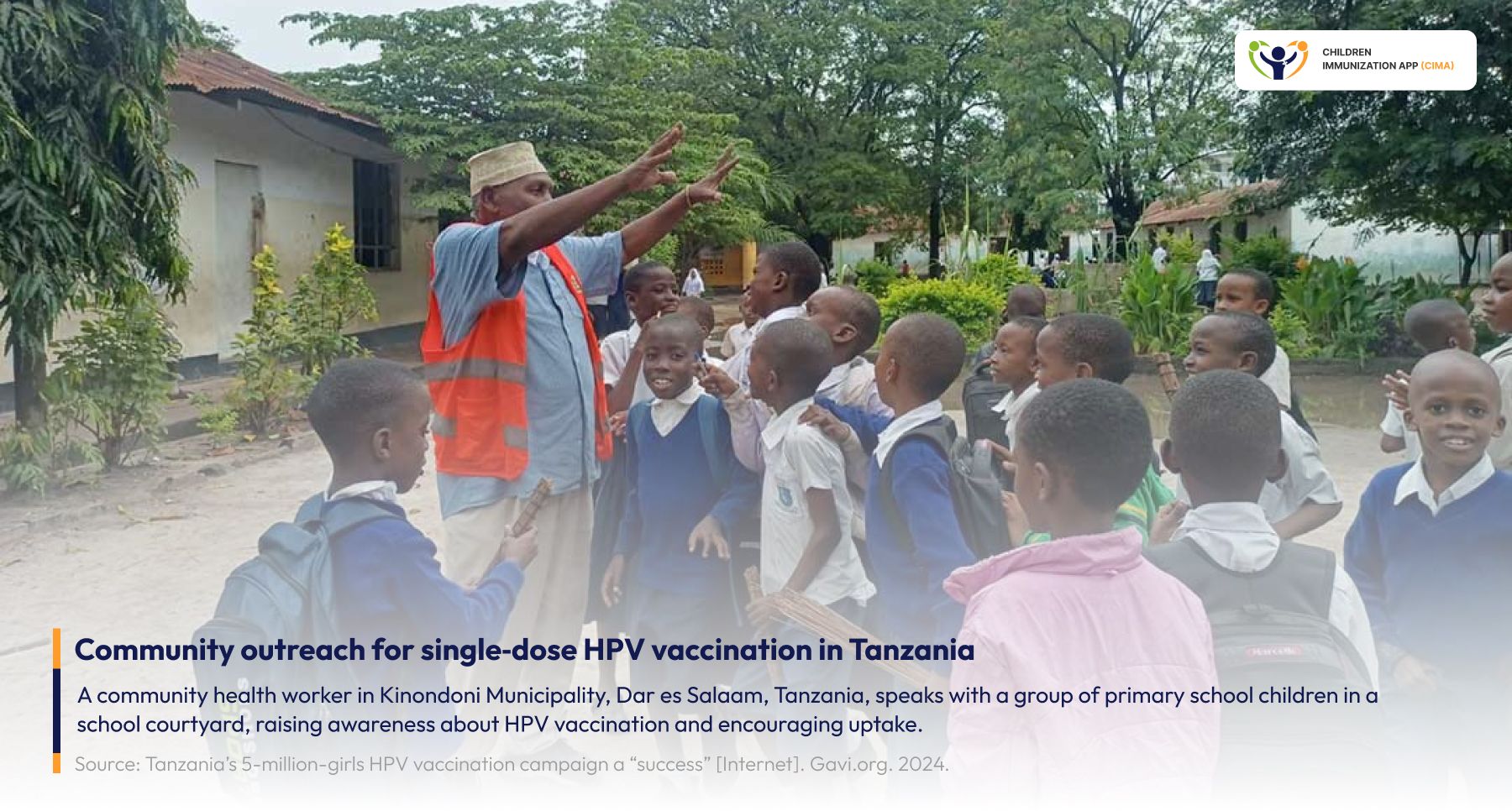
From policy to playground: Tanzania's health workers bring single-dose HPV protection to children.
The Long-Term Impact: Real-World Evidence of Cancer Prevention
A November 2025 study published in the International Journal of Cancer confirmed that the HPV vaccine provides strong, long-lasting protection against cervical disease, with effectiveness persisting for over 12 years. The population-based study showed that girls vaccinated at ages 12 or 13 experienced the greatest benefits. [15] Another 2025 review reports that girls vaccinated before age 16 were 80% less likely to have cervical cancer compared to unvaccinated girls. Critically, the review found no evidence to support claims that HPV vaccination increases the risk of serious adverse events, definitively addressing safety concerns that have fueled vaccine hesitancy. [16]
Remarkably, Scotland's research demonstrated that women from Scotland's most deprived areas benefited the most from vaccination, helping to reduce health inequalities, a finding with significant implications for equity-focused vaccination programs worldwide. [15]
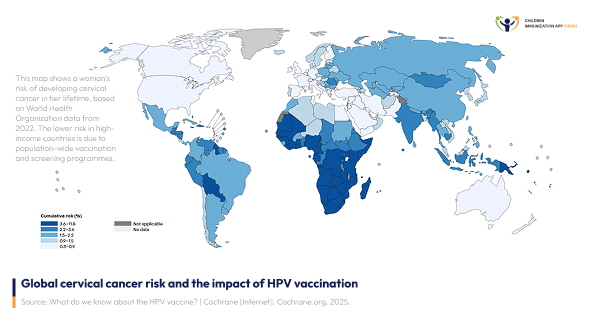
Darkest regions need HPV vaccination most—where risk is highest, the evidence-based case is clearest.
HPV Vaccination Herd Immunity Benefits
A groundbreaking 17-year study published in JAMA Pediatrics in September 2025 provided clear evidence of herd immunity from HPV vaccination. Conducted at Cincinnati Children's Hospital and involving 2,335 adolescent girls and young women, the study showed that as vaccination coverage increased from 0% to 82%, HPV infection rates dropped dramatically:
- Infections from HPV types covered by the bivalent (2‑type) vaccine fell by 98.4%.
- Infections from types covered by the quadrivalent (4‑type) vaccine dropped by 94.2%.
- Infections from types covered by the nonavalent (9‑type) vaccine declined by 75.7%.
The study demonstrated that "the vaccine indirectly protects unvaccinated people by reducing overall virus transmission," confirming population-level benefits beyond individual protection. [17]
98.4% The HPV infection drop proves it: vaccinating the many shields even those who never received a dose by reducing overall virus transmission.
The Expanding Frontier: Gender-Neutral Vaccination Strategies Gain Momentum
- 1. The case for gender‑neutral HPV vaccination by 2030
A growing global movement is calling for gender‑neutral HPV vaccination, recognizing that human papillomavirus affects everyone, not only women.
Global Action on Men’s Health and the NOMAN is an Island campaign launched a six‑point plan in September 2024 urging the World Health Organization and national governments to ensure that all countries either introduce or transition to gender‑neutral HPV vaccination (GNV) by 2030, so boys and men are routinely offered the vaccine alongside girls and women. [18]
HPV is responsible for a substantial cancer burden in men worldwide, causing many cases of penile, anal, and head and neck cancers each year, and these male cancers are rising in several regions. [19]
Advocates stress that the virus is called human papillomavirus, not “female” papillomavirus, and that with existing vaccines we already have the tools to protect everyone from HPV‑related cancers. [20]
Taken together, current evidence shows that expanding to gender‑neutral vaccination is an ethical, equitable, and pragmatic next step in global cancer prevention. [21]
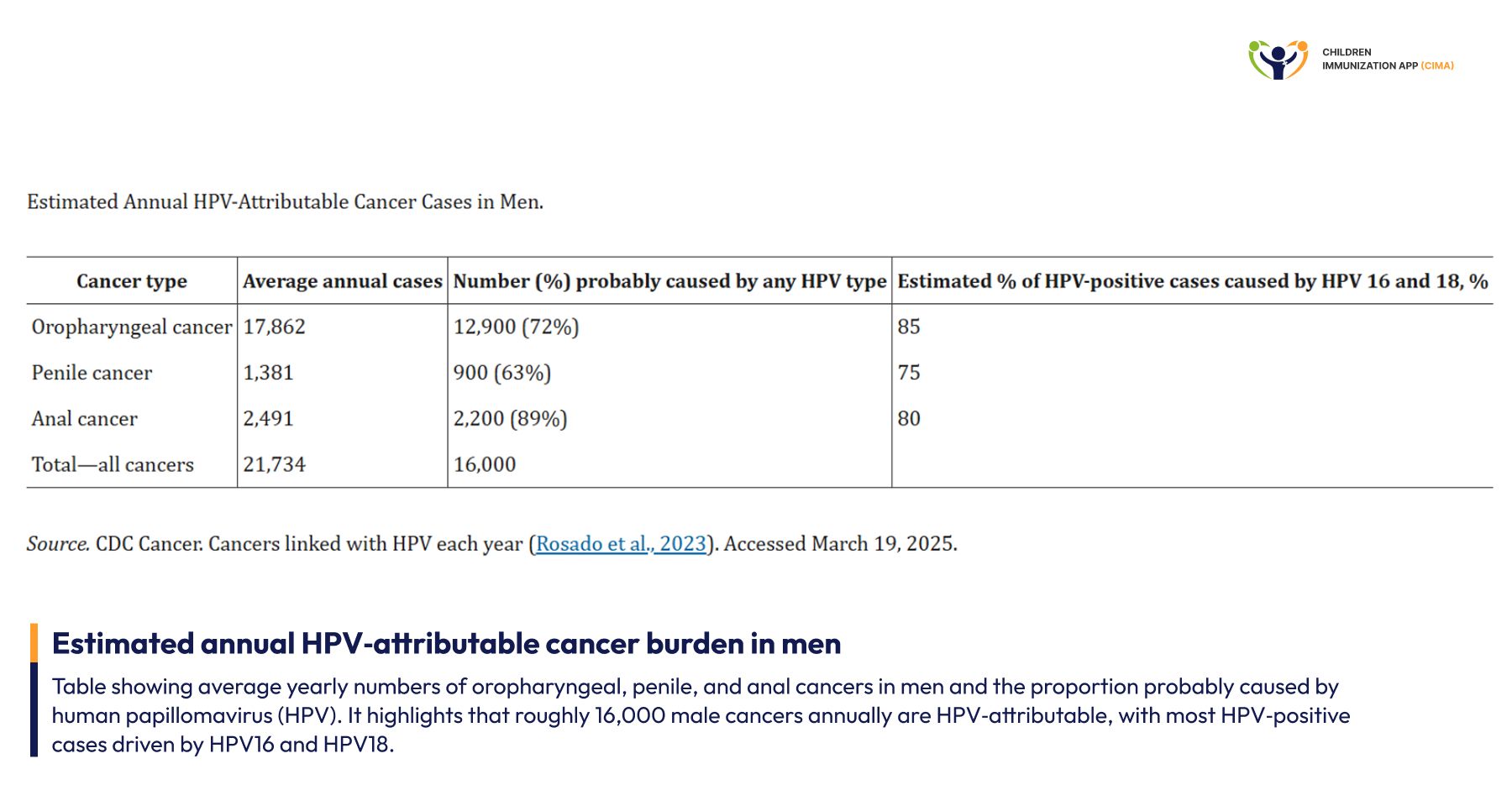
16,000 male cancer cases yearly are HPV-attributable—gender-neutral vaccination is a clinical imperative.
2. Evidence Supporting Gender-Neutral Programs
A 2024 modeling study based on Finland’s community‑randomized HPV vaccination trial found that vaccinating both boys and girls against HPV can reduce cervical cancer incidence far faster than vaccinating girls alone. According to the authors, the level of protection achieved after 8 years of gender‑neutral vaccination would require roughly 20 years of girls‑only vaccination to match. In trial communities where boys and girls were vaccinated with the bivalent HPV16/18 vaccine, the model showed a rapid and substantial drop in high‑risk HPV types, with particularly strong control of vaccine‑targeted types 16 and 18 and cross‑protected types 31 and 45.[22]
Similarly, a 2021 study in The Lancet Infectious Diseases examined anal, penile, and oral HPV infections in about 400 young men who have sex with men in Melbourne before and after Australia introduced a school‑based quadrivalent HPV vaccine program for boys in 2013. The prevalence of anal infection with vaccine‑preventable HPV types 6, 11, 16, and 18 fell from 28% in the pre‑vaccination cohort to 7% in the post‑vaccination cohort, a relative reduction of about 75%, with significant declines also seen in HPV16 and 18. The authors concluded that gender‑neutral HPV vaccination led to marked reductions in vaccine‑targeted anal HPV types in young gay and bisexual men, which is expected to lower their future risk of anal cancer. [23]
As of April 2024, 54 countries have adopted gender-neutral vaccination strategies, and this number continues to grow as the evidence base strengthens. [24]
Gender-neutral HPV vaccination achieves population-level HPV reduction in 8 years vs. 20 years with girls-only programs.
Global Implementation Progress: Expanding Access Worldwide
- 1. 159 Countries Now Include HPV Vaccination
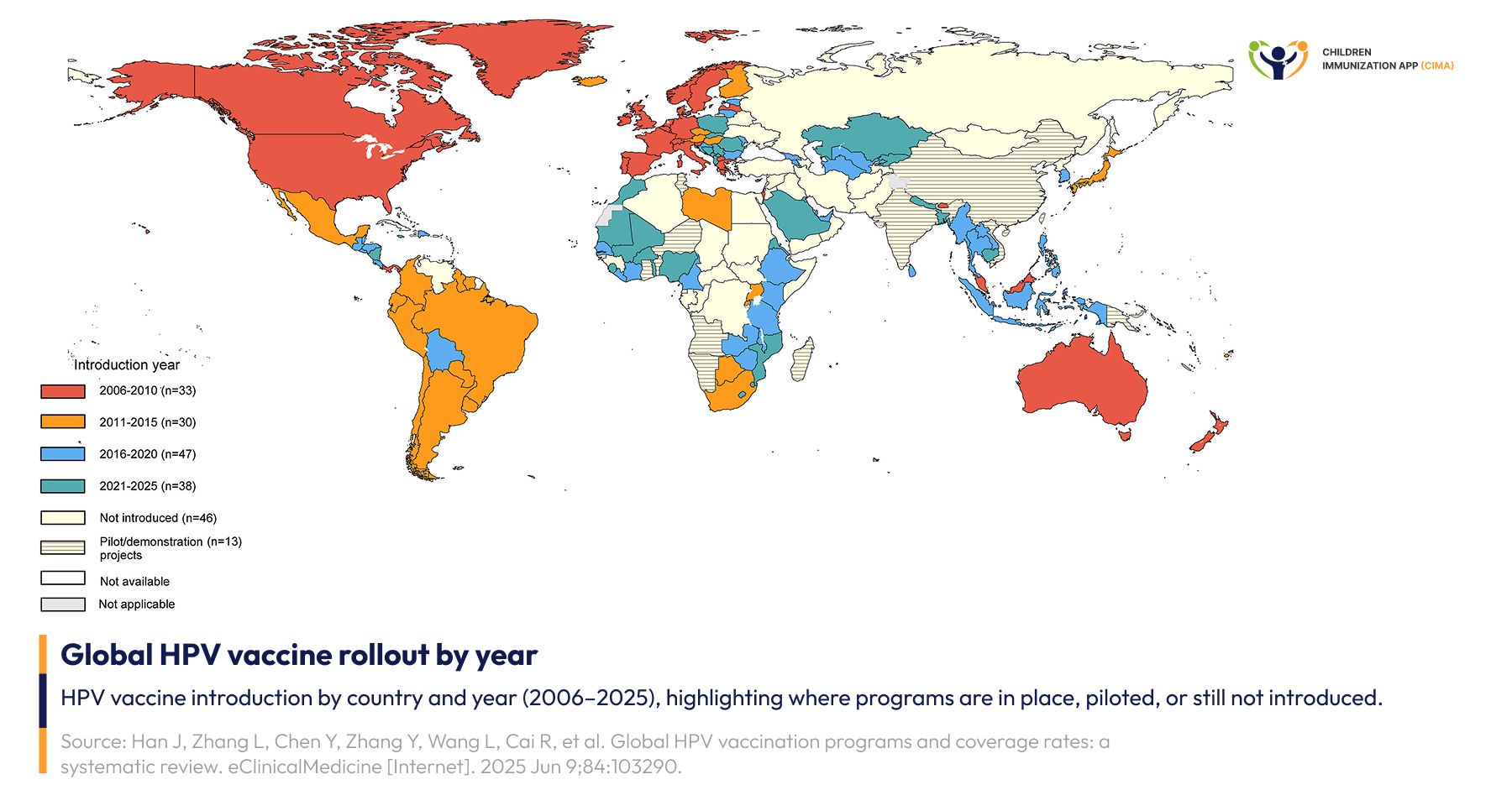
By December 2025, 159 countries (82%) have introduced HPV vaccines, representing 64% of the global population of girls aged 9-14 years. This represents remarkable progress from just 4 high-income countries that had HPV vaccines in their national schedule in 2006. https://www.tandfonline.com/doi/full/10.1080/14760584.2025.2609869
Recent introductions include:
Zimbabwe (2018)
Liberia (2019)
Mozambique (2021)
Sierra Leone (2022)
Bangladesh (2023)
Nigeria (2023)
Timor-Leste (2024)
Nepal (2025). [25]
Significant challenges remain. 14 low-income countries and 20 lower-middle-income countries still do not include HPV vaccines in national immunization programs, highlighting persistent equity gaps. [26]
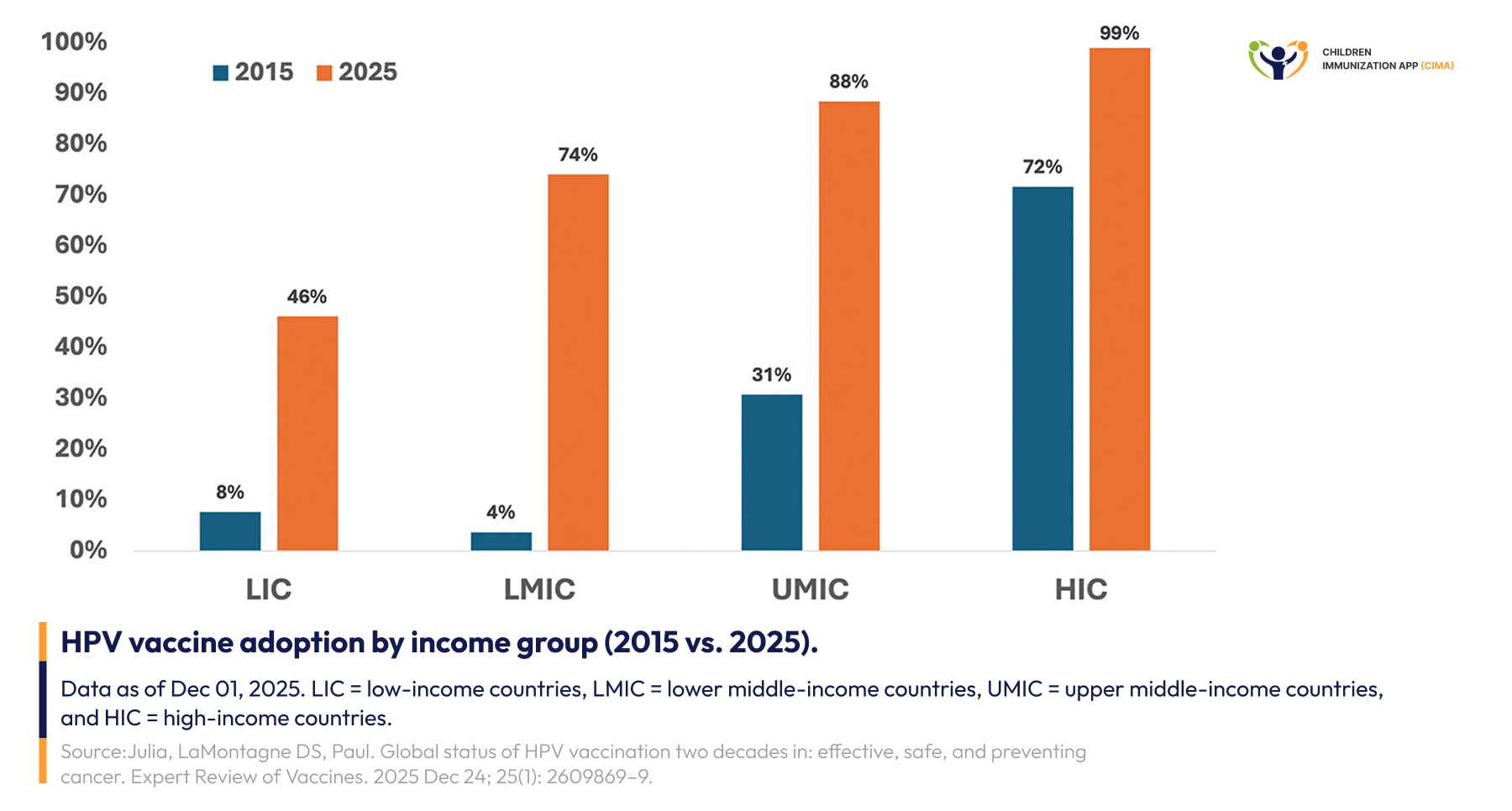
From 8% to 46% in LICs, yet HICs hit 99%—a decade of progress still shadowed by an equity gap.
2. Coverage Remains Below Targets Despite Progress
By early 2025, 148 WHO member states had added the HPV vaccine to their national immunization programs, yet coverage in the primary target group of girls aged 9–14 years remained modest, with only about 62% receiving a first dose and 48% completing the full course in 2023. Just 15 countries—around one in ten reporting nations—reached the WHO goal of 90% first‑dose coverage, and even in upper‑middle‑income countries, where uptake was highest, first‑dose coverage averaged about 72%. Overall, the researchers conclude that global HPV vaccination coverage is still far below the 90% target and that stronger, targeted strategies are urgently needed to close this gap despite encouraging declines in cervical cancer incidence in many countries. [26]
About 46 countries are yet to introduce HPV vaccination—and even adopters average only 62% first-dose coverage.
Safety Evidence: Addressing Concerns with Robust Data
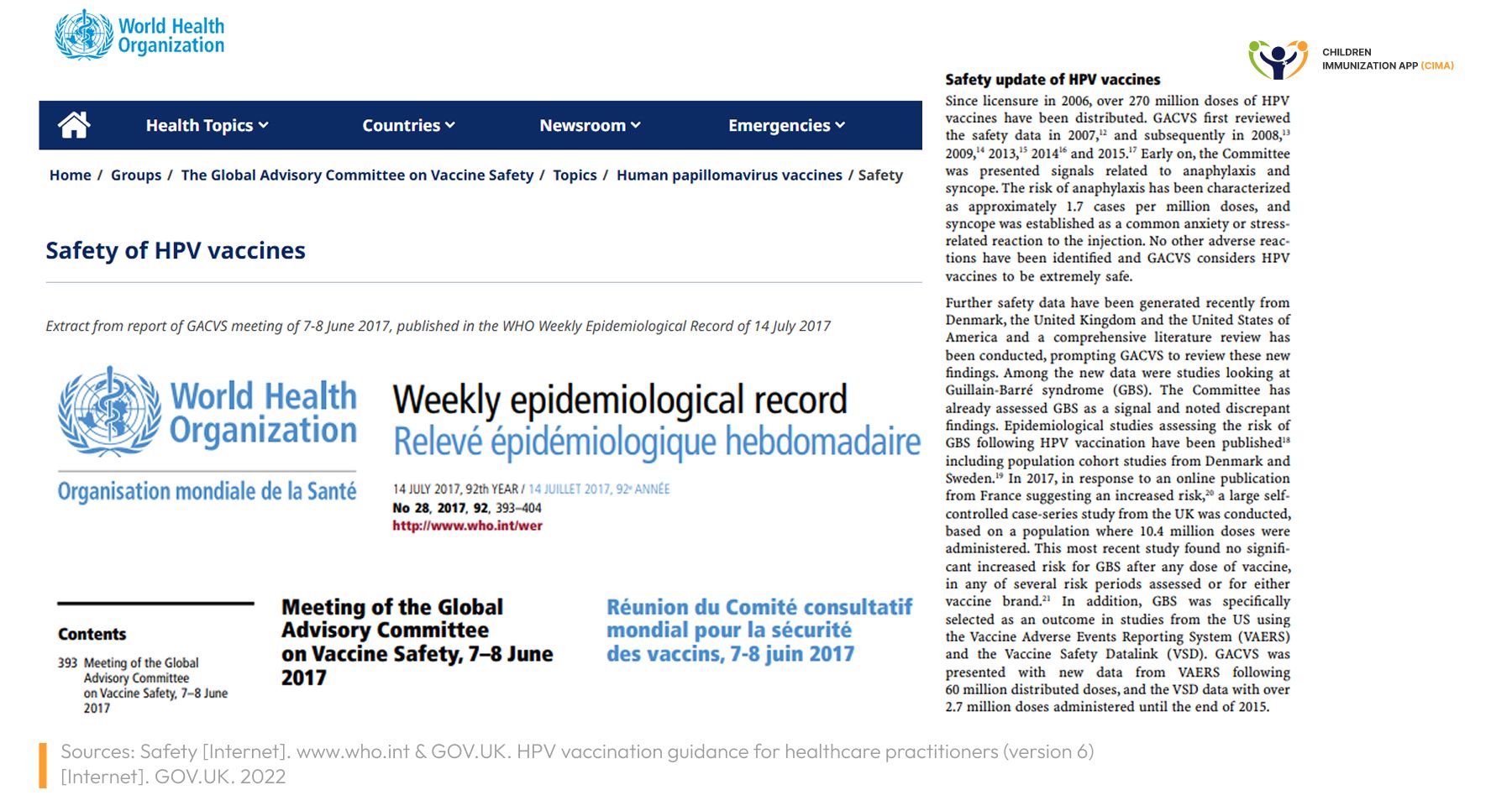
- 1. A WHO review confirms the excellent safety of HPV vaccines
WHO’s Global Advisory Committee on Vaccine Safety (GACVS) has repeatedly reviewed HPV vaccines and in its 2017 evidence review concluded that these vaccines have an excellent safety profile, with no new serious safety concerns identified despite very extensive global use. [27]
Later WHO documents (including the 2022 SAGE evidence‑to‑recommendations papers and 2023–2025 technical reviews) explicitly reaffirm those same 2017 GACVS conclusions rather than replacing them. [28]
Drawing on pharmacovigilance data from more than 175 million distributed doses at that time, GACVS found that serious adverse events such as Guillain–Barré syndrome, stroke, venous thromboembolism, seizures, or chronic fatigue syndromes occurred no more often than expected in the general population, and that the only clearly causal serious reaction was anaphylaxis at about 1–2 cases per million doses, similar to other routine vaccines. The committee therefore reaffirmed that the benefits of HPV vaccination in preventing cervical and other cancers far outweigh the very small risk of serious allergic reactions, and WHO continues to recommend HPV vaccination as a safe and effective intervention for adolescents worldwide. [27]
WHO GACVS: Millions of doses reviewed, no serious safety signals—HPV vaccine benefits far outweigh risks.
2. Common Side Effects Are Mild and Self-Limiting
The most commonly reported adverse events following HPV vaccination are local reactions:
- Pain at injection site: 80-90% of recipients (mild to moderate, resolving within 48-72 hours)
- Swelling: 20-30% of recipients (minimal and self-limiting)
- Low-grade fever: 10-15% of recipients
Serious reactions are exceedingly rare:
- Anaphylaxis: 1-2 cases per million doses
- No increased risk of autoimmune conditions, reproductive outcomes, or neurological disorders. [27 & 29]
A smile says it all—mild, brief reactions are the real story behind HPV vaccine side effects.
Practical Implications for Healthcare Providers
- 1. Vaccination Recommendations
Healthcare providers should be aware of current evidence-based recommendations:
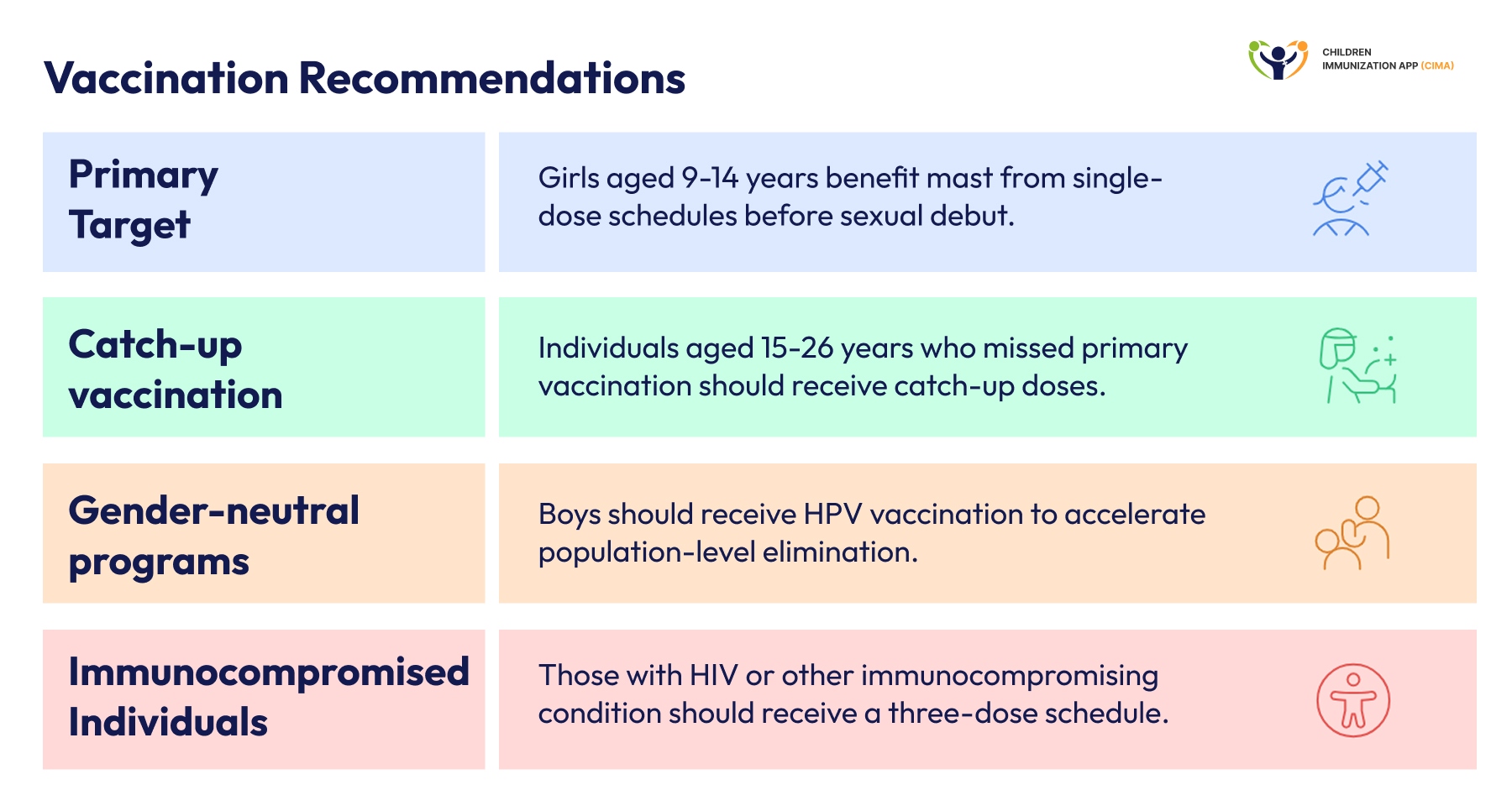
Primary target population: Girls aged 9-14 years receive the greatest benefit when vaccinated before sexual debut, with single-dose schedules now recommended by WHO.
Catch-up vaccination: Individuals aged 15-26 years who missed primary vaccination should receive catch-up doses, though efficacy is highest when vaccination occurs before exposure to HPV.
Gender-neutral programs: Where resources permit, boys should receive HPV vaccination using the same schedule as girls to accelerate population-level HPV elimination and protect against male-specific HPV cancers.
Immunocompromised individuals: Those living with HIV or other immunocompromising conditions should receive a three-dose schedule regardless of age. [30-34]
Four evidence-based rules every provider must know—from first dose timing to immunocompromised care.
Addressing Vaccine Hesitancy
Healthcare providers play a critical role in addressing vaccine hesitancy. Key evidence‑based messages include:
On safety: Global safety reviews covering more than 270 million distributed doses, together with two large Cochrane reviews including observational data, find no increased risk of serious adverse events, autoimmune disease, infertility, or neurological disorders after HPV vaccination; the main serious reaction is very rare anaphylaxis at around 1–2 cases per million doses, comparable to other routine vaccines. [27& 37]
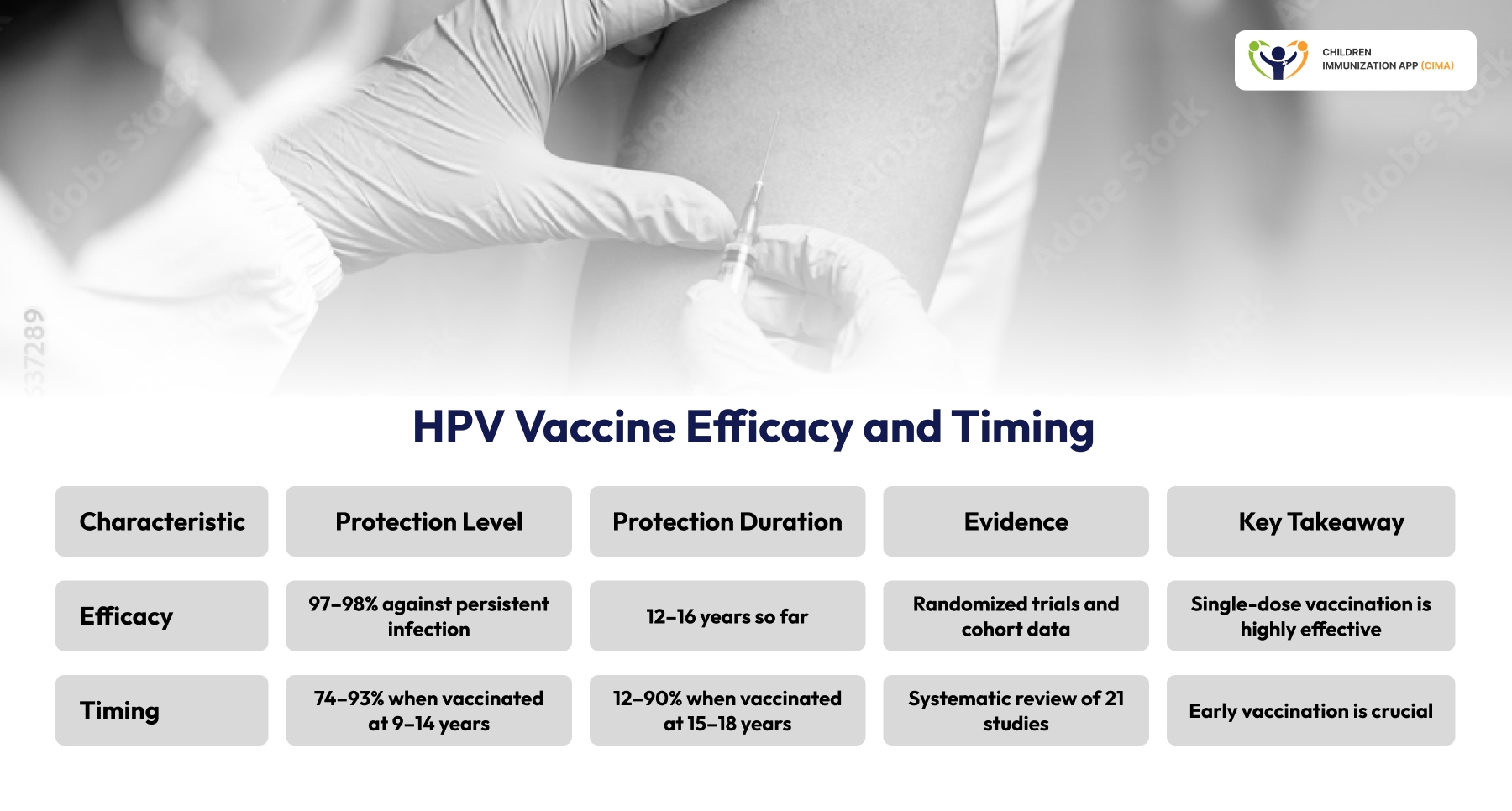
On efficacy: Randomized trials such as KEN SHE and long‑term cohort data from India and Costa Rica show that single‑dose HPV vaccination can achieve about 97–98% protection against persistent infection with key cancer‑causing types, with durable protection documented for roughly 12–16 years so far and immunologic evidence suggesting it will extend further. [4 & 8 & 9 & 15 & 38]
On equity: Population‑based evaluations of national programs (for example, in Scotland) 15 demonstrate substantial and sustained reductions in high‑grade cervical precancer and cancer, with particularly large absolute benefits in women from the most deprived areas, indicating that HPV vaccination can narrow health inequalities when high coverage is achieved in underserved communities. [15 & 39]
On timing: A 2023 systematic review of 21 studies found that HPV vaccine effectiveness was highest when vaccination occurred at ages 9–14 years, with effectiveness estimates of about 74–93% in this age group and generally lower effectiveness (about 12–90%) when vaccination was delayed to ages 15–18 years, demonstrating that HPV vaccines work best when given before sexual debut and underscoring the importance of on‑time vaccination in early adolescence. [40 & 41]
97–98% efficacy, 12–16 years durability, best at ages 9–14—the evidence that silences hesitancy.
The Path to Cervical Cancer Elimination—WHO's 90-70-90 Targets
The WHO Global Strategy to Eliminate Cervical Cancer as a Public Health Problem sets ambitious 2030 targets:
- 90% of girls fully vaccinated by age 15
- 70% of women screened with high-performance tests by ages 35 and 45
- 90% of women with cervical disease receiving appropriate treatment
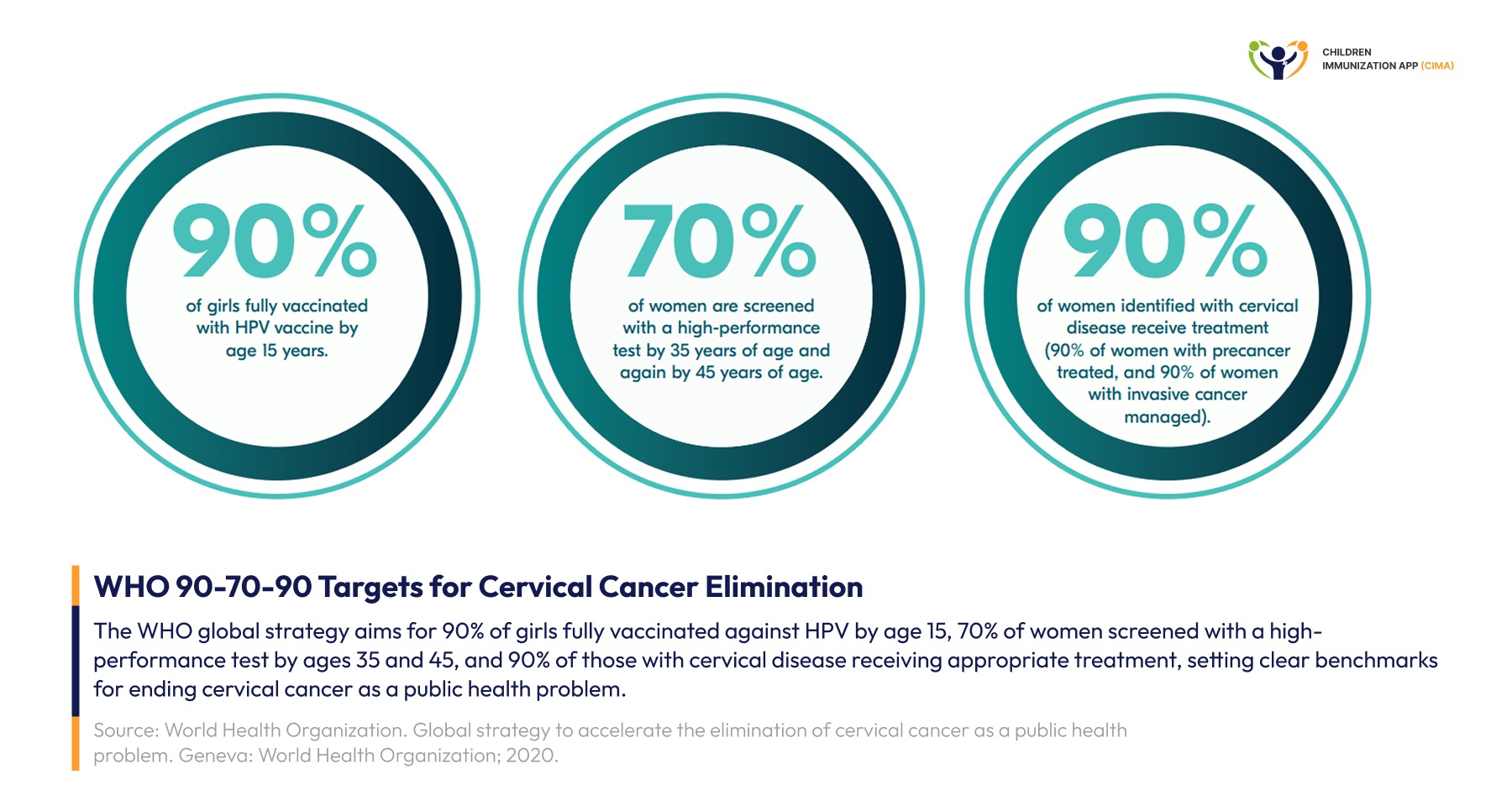
Infographic of WHO's 90-70-90 cervical cancer elimination targets: vaccinate, screen, and treat.
Conclusion: Evidence‑Based Action for the Next Generation
Taken together, today’s data show that HPV vaccination is one of the most powerful cancer‑prevention tools in modern medicine. Single-dose schedules can provide around 97–98% protection against persistent infection with the main cancer-causing types, with durable immunity now documented for 12–16 or more years, while gender-neutral programs and expanding country adoption are accelerating declines in HPV infections, precancers, and cervical cancer itself. At the same time, hundreds of millions of administered doses, rigorous WHO safety reviews, and large real‑world studies consistently confirm an excellent safety profile, with only rare serious allergic reactions and no evidence of increased autoimmune, fertility, or neurological risks.
For healthcare professionals, the mandate is practical and urgent: recommend HPV vaccination for all eligible adolescents, prioritizing vaccination before sexual debut; use clear, evidence‑based communication to counter misinformation and hesitancy; support implementation of single‑dose and gender‑neutral schedules where feasible; and champion policies that expand access in low‑coverage settings so that every girl and boy can benefit from this life‑saving protection. [1 - 36]
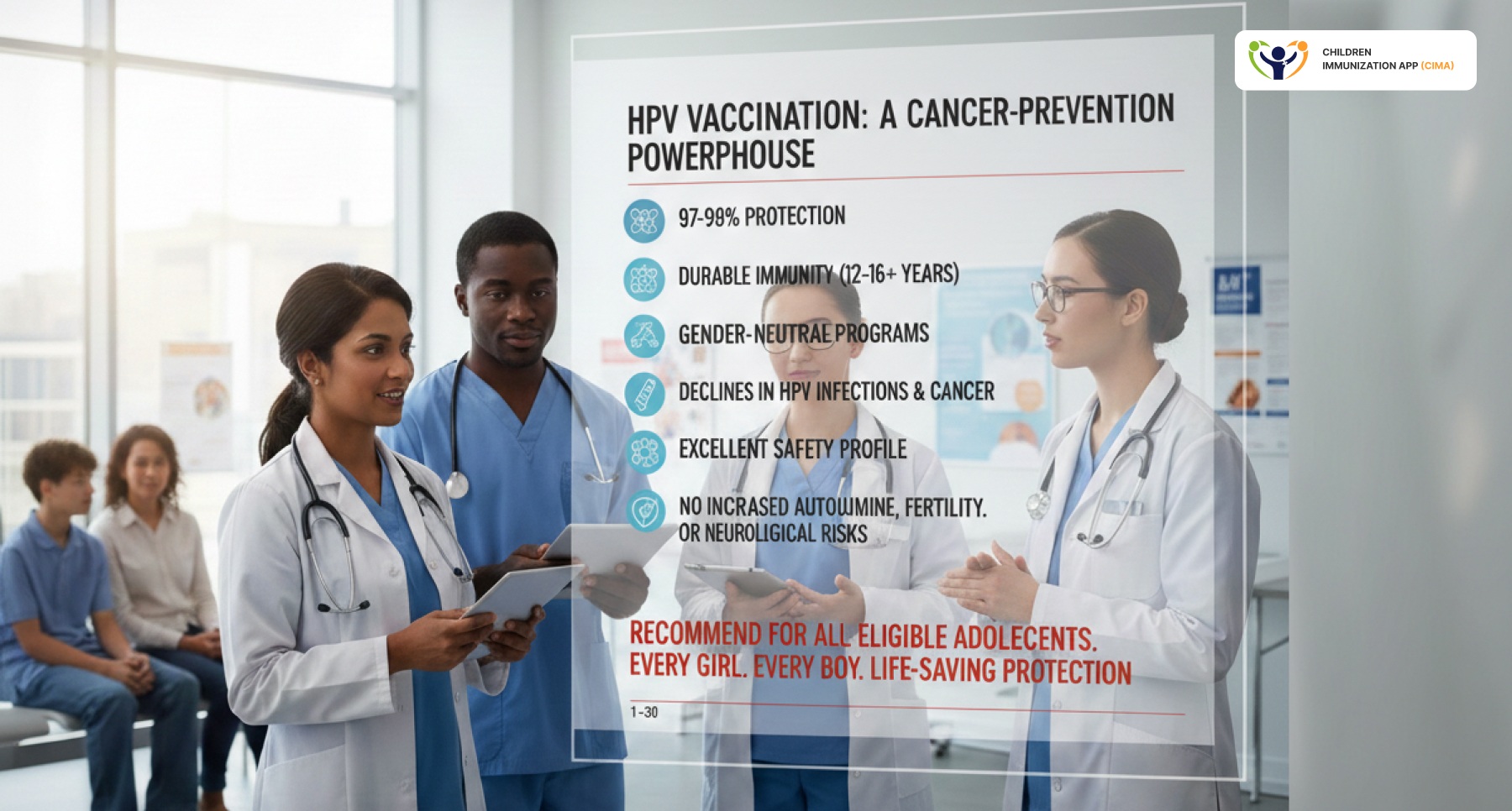
The evidence is conclusive—now providers must act: every eligible adolescent deserves life-saving HPV protection.
CIMA Health Academy: Empowering Healthcare Professionals With Cutting-Edge Knowledge
CIMA Health Academy is proud to offer Course 8: HPV Vaccination Towards Cervical Cancer Elimination, a comprehensive 34-hour training program providing healthcare professionals with the latest evidence on HPV vaccination strategies, implementation approaches, and communication techniques.
This WHO-aligned course covers:
- HPV virology, transmission dynamics, and cervical cancer epidemiology
- Vaccine types, immunological mechanisms, and safety evidence
- Program planning, delivery strategies, and cold chain management
- Communication frameworks and vaccine hesitancy management
- Prevention continuum integration and WHO elimination roadmap
With learners from 77+ countries worldwide, CIMA Health Academy has established itself as the premier global platform for vaccination and public health education, delivering over 150 hours of content totaling 11.72 CPD credits.
Visit https://www.cima.care/health-academy to explore our comprehensive vaccination courses and join healthcare professionals worldwide who are transforming cancer prevention through evidence-based practice.
Together, we can reshape cancer prevention strategies and protect the next generation from HPV-related cancers.

34 hours, 5 modules, 2.7 CPD credits—CIMA's course on the HPV vaccination program equips providers to drive cervical cancer elimination.
Image References
- 1. National Cancer Institute. HPV vaccine shown to prevent cervical cancer in Sweden study [Internet]. Cancer Currents Blog. 2020 [cited 2026 May 11]. Available from: https://www.cancer.gov/news-events/cancer-currents-blog/2020/hpv-vaccine-prevents-cervical-cancer-sweden-study
- 2. Medical Intervention and Technical Updates Organization. News category [Internet]. MITU Tanzania. [cited 2026 May 11]. Available from: https://mitu.or.tz/category/news/
- 3. Duke Kunshan University. The main types of HPV vaccines [Internet]. VaxLab. [cited 2026 May 11]. Available from: https://vaxlab.dukekunshan.edu.cn/en/evidence-db-expert/hpv-vaccine-policy-advocacy-evidence-repository/the-main-types-of-hpv-vaccines/
- 4. PubMed. Human papillomavirus vaccine-related article [Internet]. National Library of Medicine. 2024 [cited 2026 May 11]. Available from: https://pubmed.ncbi.nlm.nih.gov/38365419/
- 5. PubMed Central. HPV vaccine-related article [Internet]. National Center for Biotechnology Information. 2024 [cited 2026 May 11]. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC11555276/
- 6. Stop HPV. HPV WHO dosing recommendations brief [Internet]. 2023 [cited 2026 May 11]. Available from: https://stophpv.org/wp-content/uploads/2023/04/HPV-WHO-Dosing-Recommendations-Brief.pdf
- 7. Cochrane. What do we know about HPV vaccine? [Internet]. Cochrane. [cited 2026 May 11]. Available from: https://www.cochrane.org/about-us/news/what-do-we-know-about-hpv-vaccine
- 8. National Foundation for Infectious Diseases. HPV [Internet]. NFID. [cited 2026 May 11]. Available from: https://www.nfid.org/infectious-disease/hpv/
- 9. PubMed Central. HPV vaccination-related article [Internet]. National Center for Biotechnology Information. 2024 [cited 2026 May 11]. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12638683/
- 10. Karolinska Institutet. Gender-neutral HPV vaccination best at preventing cervical cancer [Internet]. KI News. [cited 2026 May 11]. Available from: https://news.ki.se/gender-neutral-hpv-vaccination-best-at-preventing-cervical-cancer
- 11. Taylor & Francis Online. HPV vaccine research article [Internet]. Expert Review of Vaccines. 2025 [cited 2026 May 11]. Available from: https://www.tandfonline.com/doi/full/10.1080/14760584.2025.2609869#d1e1166
- 12. The Lancet. HPV vaccine-related article [Internet]. EClinicalMedicine. 2025 [cited 2026 May 11]. Available from: https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(25)00222-6/fulltext
- 13. World Health Organization. World Health Organization official website [Internet]. WHO. [cited 2026 May 11]. Available from: https://www.who.int/
- 14. World Health Organization Regional Office for Europe. WHO-EURO-2024-5631-49185-73415 [Internet]. WHO Europe. 2024 [cited 2026 May 11]. Available from: https://www.who.int/europe/publications/i/item/WHO-EURO-2024-5631-49185-73415
- 15. Adobe Stock. Doctor hand in blue gloves holding influenza vaccine for prevention, human nurse holding syringe make injection in shoulder of patient in hospital, COVID-19 or coronavirus vaccine | Adobe Stock [Internet]. Adobe Stock. 2023 [cited 2026 May 11]. Available from: https://stock.adobe.com/images/doctor-hand-in-blue-gloves-holding-influenza-vaccine-for-prevention-human-nurse-holding-syringe-make-injection-in-shoulder-of-patient-in-hospital-covid-19-or-coronavirus-vaccine/604637289
- 16. World Health Organization. WHO publication content document [Internet]. IRIS WHO. [cited 2026 May 11]. Available from: https://iris.who.int/server/api/core/bitstreams/4e245e89-ddcc-488f-97c7-9de5e08524ef/content
Blog Resources
- 1- Ghosh A, Chatterjee S, Dawn A, Das A. HPV Vaccines – An Overview. Indian Journal of Dermatology [Internet]. 2025 Jun 30;70(4):188–200. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12306887/2- Miazga W, Tatara T, Gujski M, Pinkas J, Ostrowski J, Religioni U. Global Guidelines and Trends in HPV Vaccination for Cervical Cancer Prevention. Medical Science Monitor [Internet]. 2025 Mar 6;31. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12039458/
- 3- Man I, Georges D, Basu P, Baussano I. Leveraging single-dose human papillomavirus vaccination dose-efficiency to attain cervical cancer elimination in resource-constrained settings. JNCI Monographs [Internet]. 2024 Oct 1;2024(67):400–409. Available from: https://doi.org/10.1093/jncimonographs/lgae035
- 4- Ben-Ari E. One HPV vaccine dose prevents cancer-causing infections - NCI [Internet]. 2022. Available from: https://www.cancer.gov/news-events/cancer-currents-blog/2022/cervical-cancer-hpv-vaccine-one-dose-kenya
- 5- Barnabas RV, Brown ER, Onono MA, Bukusi EA, Njoroge B, Winer RL, et al. Durability of single-dose HPV vaccination in young Kenyan women: randomized controlled trial 3-year results. Nature Medicine [Internet]. 2023 Dec 1;29(12):3224–3232. Available from: https://www.nature.com/articles/s41591-023-02658-0
- 6- Baisley K, Kemp TJ, Mugo NR, Whitworth H, Onono MA, Njoroge B, et al. Comparing one dose of HPV vaccine in girls aged 9–14 years in Tanzania (DoRIS) with one dose in young women aged 15–20 years in Kenya (KEN SHE): an immunobridging analysis of randomized controlled trials. The. Lancet Global health/The lancet Global health. 2024 Mar 1; 1;12(3):e491–9.
- 7- Porras C, Romero B, Hernández BY, Herrero R, Rodríguez AC, Safaeian M, et al. HPV16/18 antibodies 16-years after single dose of bivalent HPV vaccination: Costa Rica HPV vaccine trial. J Natl Cancer Inst Monogr. 2024;2024(67):329-336.
- 8- Malvi SG, Esmy PO, Muwonge R, Joshi S, Poli URR, Lucas E, et al. A prospective cohort study comparing efficacy of 1 dose of quadrivalent human papillomavirus vaccine to 2 and 3 doses at an average follow up of 12 years postvaccination. Journal of the National Cancer Institute Monographs [Internet]. 2024 Jan;2024(67):317–28. Available from: https://pubmed.ncbi.nlm.nih.gov/39529521/
- 9- World Health Organization. Human papillomavirus vaccines: WHO position paper, December 2022 [Internet]. www.who.int. 2022. Available from: https://www.who.int/publications/i/item/who-wer9750-645-672
- 10- One-dose Human Papillomavirus (HPV) vaccine offers solid protection against cervical cancer - PAHO/WHO | Pan American Health Organization [Internet]. www.paho.org. Available from: https://www.paho.org/en/news/11-4-2022-one-dose-human-papillomavirus-hpv-vaccine-offers-solid-protection-against-cervical
- 11- One Dose at a Time: Mobilizing to Eliminate Cervical Cancer in Nigeria | International Vaccine Access Center [Internet]. publichealth.jhu.edu. 2024. Available from: https://publichealth.jhu.edu/ivac/2024/one-dose-at-a-time-mobilizing-to-eliminate-cervical-cancer-in-nigeria
- 12- Tanzania’s 5-million-girls HPV vaccination campaign a “success” [Internet]. Gavi.org. 2024. Available from: https://www.gavi.org/vaccineswork/tanzanias-5-million-girls-hpv-vaccination-campaign-success
- 13- Kenya embraces single-dose HPV vaccine as cervical cancer deaths remain high [Internet]. Standardmedia.co.ke. 2026. Available from: https://www.standardmedia.co.ke/health/health-science/article/2001540513/kenya-embraces-single-dose-hpv-vaccine-as-cervical-cancer-deaths-remain-high
- 14- HPV Vaccine (Human Papillomavirus Vaccine) [Internet]. vaccineknowledge.ox.ac.uk. Available from: https://vaccineknowledge.ox.ac.uk/hpv-vaccine#Key-facts-about-the-HPV-Vaccine
- 15- Palmer TJ, Kavanagh K, Cuschieri K, Cameron RL, Graham C, Wilson A, et al. Sustained impact of bivalent HPV immunisation on CIN incidence over two rounds of cervical screening. International Journal of Cancer. 2025 Nov 3;158(5):1348–60.
- 16- Parkinson M. New research confirms HPV vaccination prevents cervical cancer | Cochrane [Internet]. Cochrane.org. 2025. Available from: https://www.cochrane.org/about-us/news/new-research-confirms-hpv-vaccination-prevents-cervical-cancer
- 17- Study shows HPV vaccine protects vaccinated and unvaccinated women [Internet]. Prnewswire.com. 2026. Available from: https://www.prnewswire.com/news-releases/study-shows-hpv-vaccine-protects-vaccinatedand-unvaccinatedwomen-302568507.html
- 18- Boys, Men and HPV - GLOBAL ACTION ON MEN’S HEALTH [Internet]. gamh.org. 2024. Available from: https://gamh.org/boys-men-hpv/
- 19- Lipsky MS, Gunnell B, Nguyen J, Lee S, Wolfe G, Hung M. HPV Prevention in Men: A Narrative Review of Strategies, Risks, and Public Health Implications. American Journal of Men’s Health. 2025 Nov;19(6).
- 20- Allen F. Call for global gender-neutral HPV vaccination by 2030 [Internet]. The Microbiologist. 2024. Available from: https://www.the-microbiologist.com/news/call-for-global-gender-neutral-hpv-vaccination-by-2030/4093.article
- 21- Luo Q, Ni Q. Gender-neutral human papillomavirus vaccination: an equitable and cost-effective public health investment. Frontiers in Public Health. 2026 Jan 5;13.
- 22- Naidoo D, Govender K, Mantell JE. Breaking barriers: why including boys and men is key to HPV prevention. BMC Medicine. 2024 Nov 8;22(1).
- 23- Chow EPF, Tabrizi SN, Fairley CK, Wigan R, Machalek DA, Garland SM, et al. Prevalence of human papillomavirus in young men who have sex with men after the implementation of gender-neutral HPV vaccination: a repeated cross-sectional study. Lancet Infectious Diseases. 2021 Oct;21(10):1448–57.
- 24- Schuind AE, Balaji KA, Du A, Yuan Y, Dull P. Human papillomavirus prophylactic vaccines: update on new vaccine development and implications for single-dose policy. Journal of the National Cancer Institute Monographs [Internet]. 2024 Jan;2024(67):410–16. Available from: https://pubmed.ncbi.nlm.nih.gov/39529522/
- 25- Julia, LaMontagne DS, Paul. Global status of HPV vaccination two decades in: effective, safe and preventing cancer. Expert Review of Vaccines. 2025 Dec 24;25(1):2609869–9.
- 26- Han J, Zhang L, Chen Y, Zhang Y, Wang L, Cai R, et al. Global HPV vaccination programs and coverage rates: a systematic review. eClinicalMedicine [Internet]. 2025 Jun 9;84:103290. Available from: https://www.sciencedirect.com/science/article/pii/S2589537025002226
- 27- Safety [Internet]. www.who.int. Available from: https://www.who.int/groups/global-advisory-committee-on-vaccine-safety/topics/human-papillomavirus-vaccines/safety
- 28- GOV.UK. HPV vaccination guidance for healthcare practitioners (version 6) [Internet]. GOV.UK. 2022. Available from: https://www.gov.uk/government/publications/hpv-universal-vaccination-guidance-for-health-professionals/hpv-vaccination-guidance-for-healthcare-practitioners
- 29- World Health Organization. Questions and answers about human papillomavirus (HPV) vaccine [Internet]. Geneva: WHO; 2017 [cited 2026 Feb 15]. Available from: https://cdn.who.int/media/docs/librariesprovider2/default-document-library/who-hpv-qa.pdf
- 30- World Health Organization. Human papillomavirus vaccines: WHO position paper, December 2022 [Internet]. www.who.int. 2022. Available from: https://www.who.int/publications/i/item/who-wer9750-645-672
- 31- People with immunocompromising conditions are recommended to receive 3 doses of HPV vaccine [Internet]. The Australian Immunisation Handbook. 2023. Available from: https://immunisationhandbook.health.gov.au/recommendations/people-with-immunocompromising-conditions-are-recommended-to-receive-3-doses-of-hpv-vaccine
- 32- Luo Q, Ni Q. Gender-neutral human papillomavirus vaccination: an equitable and cost-effective public health investment. Frontiers in Public Health. 2026 Jan 5;13.
- 33- WHO. Human papillomavirus (HPV) [Internet]. www.who.int. 2022. Available from: https://www.who.int/teams/immunization-vaccines-and-biologicals/diseases/human-papillomavirus-vaccines-(HPV)
- 34- WHO. WHO updates recommendations on HPV vaccination schedule [Internet]. www.who.int. 2022. Available from: https://www.who.int/news/item/20-12-2022-WHO-updates-recommendations-on-HPV-vaccination-schedule
- 35- Ghosh A, Chatterjee S, Dawn A, Das A. HPV Vaccines – An Overview. Indian Journal of Dermatology [Internet]. 2025 Jun 30;70(4):188–200. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12306887/
- 36- Kim J, Choe YJ, Park J, Cho J, Cheong C, Oh JK, et al. Comparative Effects of Bivalent, Quadrivalent, and Nonavalent Human Papillomavirus Vaccines in The Prevention of Genotype-Specific Infection: A Systematic Review and Network Meta-Analysis. Infection & Chemotherapy. 2024;56(1):37–7. Available from: https://doi.org/10.3947/ic.2023.0064
- 37- Infertility [Internet]. www.who.int. Available from: https://www.who.int/groups/global-advisory-committee-on-vaccine-safety/topics/human-papillomavirus-vaccines/infertility
- 38- Barnabas R. A randomized trial of single-dose HPV vaccination efficacy among young women: Month 54 durability results [Internet]. CDC ACIP slides. Available from: https://www.cdc.gov/acip/downloads/slides-2025-04-15-16/03-Barnabas-HPV-508.pdf
- 39- New study shows long-term effectiveness of HPV vaccine | University of Strathclyde [Internet]. Strath.ac.uk. Available from: https://www.strath.ac.uk/whystrathclyde/news/2025/newstudyshowslong-termeffectivenessofhpvvaccine/
- 40- Ellingson MK, Sheikha H, Nyhan K, Oliveira CR, Niccolai LM. Human papillomavirus vaccine effectiveness by age at vaccination: A systematic review. Human vaccines & immunotherapeutics [Internet]. 2023;19(2):2239085. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10399474/
- 41- Mehran Rostami Varnousfaderani, Zahedeh Khoshnazar, Hamidreza Zeratie, Parisa Hosseini Koukamari. Optimizing HPV vaccine effectiveness: impact of vaccination age and dose schedule on immunogenicity and cervical cancer prevention. Frontiers in Public Health. 2025 May 7;13.
Enjoyed this article?
Share it with your friends on LinkedIn: HPV Vaccination Evidence: Single-Dose Efficacy, Proven Safety, Optimal Timing, and Insights to Address Vaccine Hesitancy![]()
Follow us on LinkedIn for more updates and insights: Cima Care GmbH ![]()