Effective Zero-Dose Solutions: CIMA Care, an Evidence-Based Digital Platform Delivering Proven, Affordable Immunization Coverage with Reduced Defaulter Rates |
February 05, 2026 . 7 Minutes read
Bridging the Immunization Gap: How Digital Innovation Delivers Cost-Effective Solutions for Zero-Dose Children
The Global Challenge of Zero-Dose Children
Despite recent progress, the global immunization gap remains substantial: in 2024, 19.9 million infants missed at least one dose of a DTP-containing vaccine. Of these, 14.3 million were completely unvaccinated, zero-dose children, a figure that exceeds the Immunization Agenda 2030 trajectory by 4 million and is 1.4 million higher than the 2019 baseline. Another 5.6 million infants received some, but not all required doses. Critically, roughly 55 percent of these 19.9 million un- or under-vaccinated children are concentrated in only ten countries, including Ethiopia. [1]
14.3M zero-dose infants: Health workers extend vaccination to pastoralist families.
Understanding the Ethiopian Context: A Rigorous Cost Analysis
Ethiopia has invested heavily in strengthening its Expanded Programme on Immunization by training large numbers of health extension workers and creating 15,000 health posts. These efforts have improved access, yet a substantial gap remains. From 2019 to 2021, about 1.1 million Ethiopian children received no vaccines at all. The 2019 Demographic and Health Survey similarly found that 19 percent of children were completely unvaccinated, with almost half of this zero-dose population residing in the Oromia region. [2] Oromia is Ethiopia's largest provincial state, located in the central part of the country, and it serves as the land of the Oromo people, with its capital in Addis Ababa (Finfinne). [7]
A comprehensive study conducted from December 2023 to November 2024 examined the costs of reaching zero-dose children across multiple immunization delivery strategies (from 49 facilities) in Ethiopia's Afar and Somali regions. All costs were converted from Ethiopian birr to 2024 USD, and results are presented as cost per vaccine dose delivered and per zero-dose child reached. This research, conducted by Fenot Associates and ThinkWell, provides critical insights into the economics of vaccination delivery in challenging contexts. [3]

Ethiopian healthcare worker displays a vaccine amid the national flag—reaching 1.1M zero-dose children.
The Ethiopian study, the Strategies Assessed
The Ethiopian study evaluated three primary delivery approaches:
- 1- Routine Immunization and Regular Outreach (RI/RO): Facility-based services delivered five days per week at health centers and 1-2 days at health posts (provided the majority of vaccine doses), supplemented by weekly outreach from health posts and monthly outreach from health centers.
Health posts are the lowest-level, community-based health facilities, typically located in rural and pastoralist areas and staffed by frontline health workers who supply more doses overall at a lower average monthly cost, while health centers are supervisory and referral points with wider catchment areas and more comprehensive services and deliver fewer doses but at a higher monthly cost and with greater resource intensity. - 2- Periodic Intensification of Routine Immunization (PIRI): Campaign-style immunization activities designed to deliver routine vaccinations in low-coverage districts, planned for implementation four times annually. It is designed to target populations that were previously missed or underserved.
- 3- Mobile Health and Nutrition Teams (MHNTs): Integrated service delivery teams equipped with dedicated vehicles traveling to remote communities 5-6 days per week, providing immunization alongside nutrition, maternal health, and treatment services. [3]
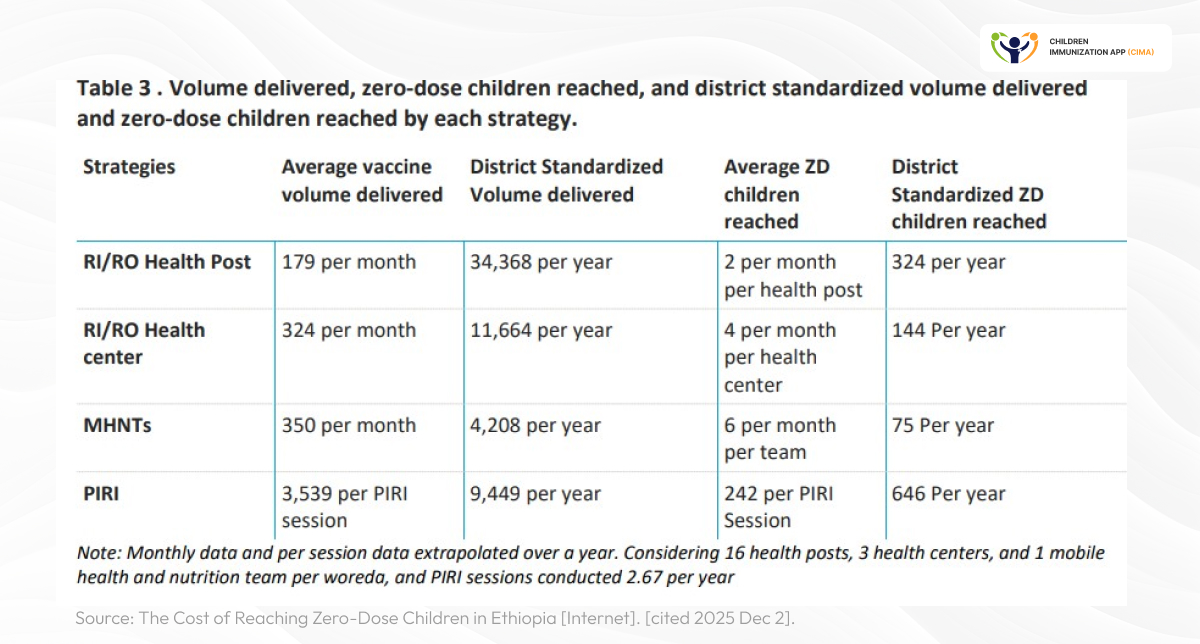
Four immunization strategies compared: PIRI reaches 242 zero-dose children per session annually.
The Cost Reality: What It Takes to Reach Every Child
The Ethiopian study revealed significant variation in the cost-effectiveness of different approaches, particularly when analyzing the cost per zero-dose (ZD) child reached:
Cost Per Zero-Dose Child Reached (Economic Costs):
PIRI campaigns: $6.65 (reaching 646 children per year per district)
PIRI is the most cost-efficient strategy for reaching ZD, Zero Dose children. This low cost is achieved because PIRI effectively targets ZD populations (64% of Penta1 doses went to ZD children). Penta1 is the acronym used for the first dose of the Diphtheria, Tetanus, and Pertussis-Containing Vaccine (DTP1). In the context of the zero-dose (ZD) study, Penta1 is the critical metric for defining zero-dose children, who are infants that have not received this first dose by the end of their first year of life. The immunization-specific cost is only $4.29 per ZD child. PIRI is largely driven by financial costs, primarily per diem and travel allowances.Health posts (RI/RO): $52.47(reaching 324 children per year per district)
Health posts deliver the majority of total vaccine doses (34,368 doses per year). Within the RI/RO strategy, regular outreach is more cost-efficient for ZD children. Major cost drivers are paid for labor and cold chain equipment.Health centers (RI/RO): $90.40 (reaching 144 children per year per district)
Health centers have the highest cost per ZD child among facility-based strategies, reflecting the limitations of facility-based routine immunization in actively tracking and reaching ZD children. Opportunity costs (resources used for immunization activities that do not represent a direct, immediate financial expenditure but contribute to the total economic cost of the strategy), with drivers including paid labor, cold chain equipment, and vehicles, dominate costs.MHNTs: $129.26 (reaching 75 children per year per district, including comprehensive health services)
This figure represents the highest overall cost per ZD child, mainly due to high shared program expenses. MHNTs integrate vaccination with high-demand services like nutrition and rely heavily on costs for staff, vehicles, and transport/fuel.
These findings align with broader evidence from multiple countries. Recent syntheses of zero-dose interventions show that supplemental or campaign-style strategies that reach large numbers of zero-dose children in a single round often have a lower cost per dose or per child reached compared with routine services, but because they are periodic rather than continuous, they can result in children remaining off-schedule for longer intervals between doses and relying less on routine immunization contacts. [4-6]
Key Finding: PIRI emerged as the most cost-efficient approach for reaching zero-dose children in Ethiopia's pastoralist regions (areas where communities rely mainly on livestock herding and tend to be mobile or nomadic, often living in remote locations with little access to fixed health facilities), with 64% of vaccinations administered through PIRI going to previously unvaccinated children, a proportion significantly higher than for other approaches. [3]
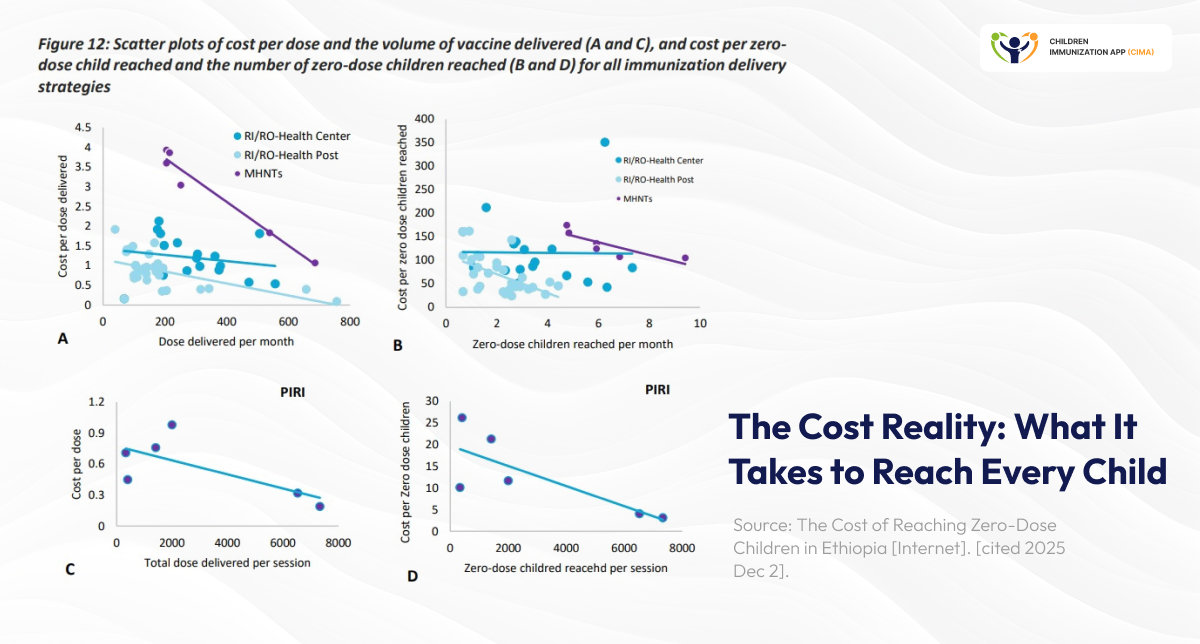
Cost efficiency revealed: PIRI at $6.65 per child outperforms all strategies in scatter analysis.
The Sustainability Challenge: Beyond Unit Costs
While PIRI demonstrated impressive cost-efficiency, the Ethiopian study identified critical sustainability concerns:
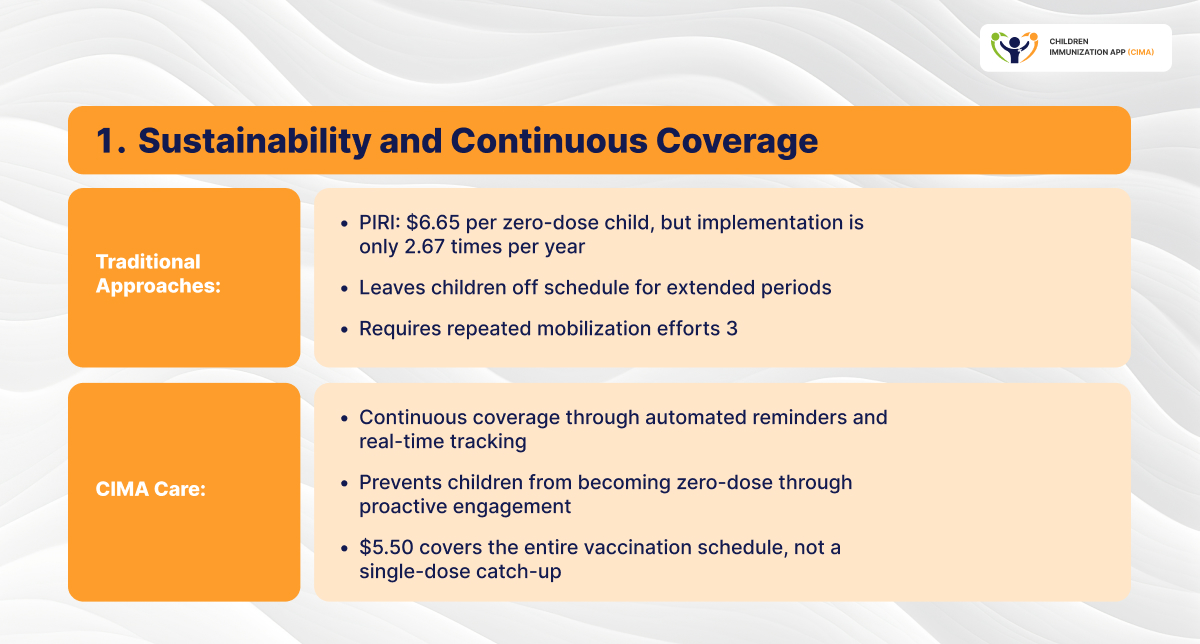
- 1- Frequency dependence: PIRI's low unit cost partly results from infrequent implementation (averaging 2.67 sessions annually rather than the planned four), allowing zero-dose children to accumulate between rounds.
- 2- Limited Long-term Effectiveness in Pastoralist Areas: The predominantly pastoralist lifestyle in the study areas (Afar and Somali) makes follow-up difficult, and many children are missed between campaigns, which limits PIRI's long-term effectiveness. PIRI may therefore be most beneficial in settled communities.
- 3- Integration gaps: Qualitative findings revealed that many parents wait for the next PIRI campaign rather than seeking routine services, contributing to dropout rates and delays in complete immunization.
- 4- Partner dependency: PIRI implementation heavily depends on external partner support, with varying intensity across districts based on funding availability.
- 5- Financial Reliance on Direct Expenditure: PIRI relies on substantial direct financial expenditure (financial costs) rather than relying predominantly on existing health system resources (opportunity costs). 63% of PIRI's economic cost is financial.
- 6- Budget Transparency Issues: Qualitative findings suggest that budget allocation for PIRI is less transparent compared to other strategies.
- 7- Context specificity: Unit costs varied significantly across districts and facilities, with costs in the more sparsely populated Afar region exceeding those in the Somali region despite similar overall program costs.
- 8- Risk of Duplication: Simultaneous implementation of PIRI and MHNTs (Mobile Health and Nutrition Teams) in the same area may lead to resource duplication and reduced effectiveness, underscoring the need for careful planning. [3]

PIRI's sustainability cycle: 2.67 annual sessions and 63% financial costs create dependencies.
CIMA Care: A Comprehensive Digital Platform
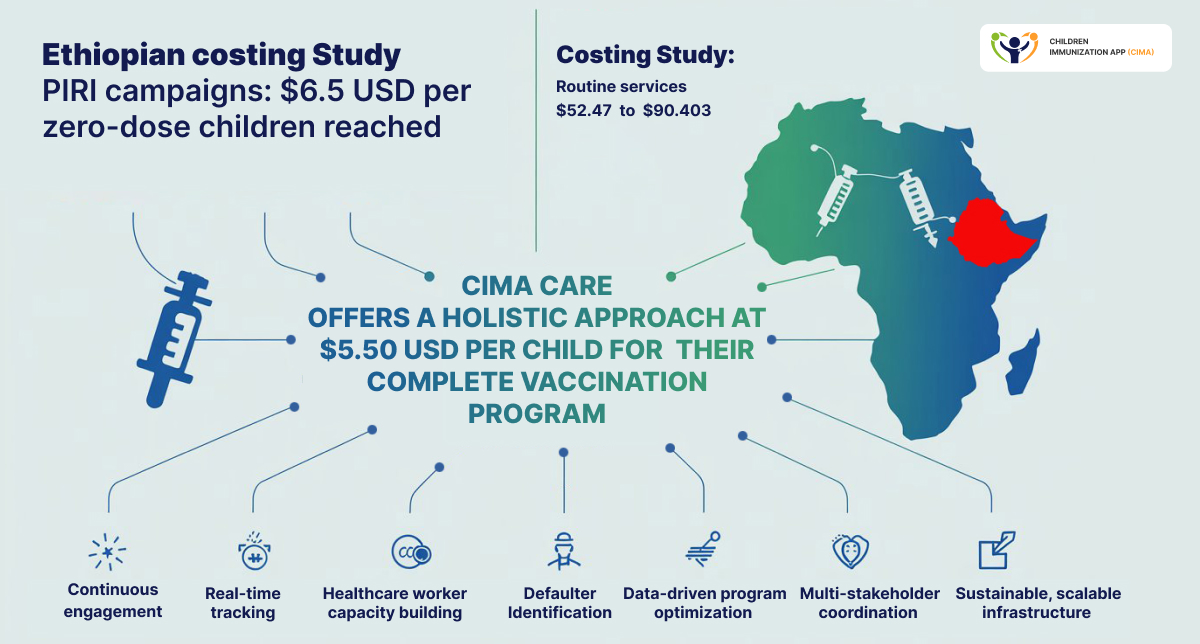
CIMA Care offers a holistic approach at $5.50 USD per child for their complete vaccination program—a cost structure that compares favorably with all traditional delivery strategies assessed in Ethiopia while providing sustainable, continuous coverage. [19]
What This Investment Includes:
- For Parents and Communities:
- Educational messaging addressing vaccine concerns and combating misinformation
- Automated SMS vaccination reminders
- Engagement with community health workers for personalized support and defaulter tracing
- For Healthcare Providers:
- Accredited professional development courses for nurses and healthcare staff
- Advanced clinic dashboard for real-time vaccination tracking
- Comprehensive data analytics and visualization tools
- Technical support and system integration
- For Health Authorities:
- Real-time defaulter tracking and monitoring systems
- Advanced analytics dashboards for evidence-based decision-making
- Resource optimization insights
- Strategic planning tools for targeted interventions [19]
CIMA Care platform at $5.50 per child—undercutting PIRI's $6.65 with continuous digital coverage.
Evidence of Impact
CIMA Care's effectiveness has been documented across multiple challenging contexts:
- 23% improvement in vaccination coverage in Cameroon [8]
- 19% improvement in Jordan's Zaatari Refugee Camp [9]
- Successful deployment in refugee camps and national health systems across multiple countries
- Improved vaccination timeliness, uptake, and completion rates
- Effective support for mobile and refugee populations with maintained documentation [8-12]
- UNODC recognized CIMA Care for integrating its parenting tips into the CIMA vaccination app in Cameroon, highlighting the impact of using technology to support children and families in challenging environments. [13]
- The CIMA app is endorsed as a best-practice model for comprehensive immunization in vulnerable populations, cited in Li et al.'s landmark 2025 scoping review (Children journal). [14]
CIMA Care's proven impact: peer-reviewed research & UN recognition across refugee & national systems.
CIMA: Advanced Technical Capabilities
CIMA Care's technical features address the specific challenges identified in the Ethiopian study:
- Offline functionality: Ensures uninterrupted service in areas with limited connectivity, a critical feature for regions like Afar and Somali
- Multi-language support: Available in English, French, and Arabic
- Data security: Robust encryption compliant with international healthcare standards
- Interoperability: Seamless integration with existing health information systems [19]

CIMA's tech bridging gaps: offline access, multilingual interface & secure data for remote regions.
Comparative Cost-Effectiveness Analysis
When comparing CIMA Care's $5.50 per child to Ethiopia's strategy costs, several critical advantages emerge:
Cost comparison: CIMA's $5.50 delivers continuous coverage vs. traditional $6.65 one-time outreach.
Beyond delivery: CIMA's $5.50 includes training, tracking, & insights missing from traditional costs.
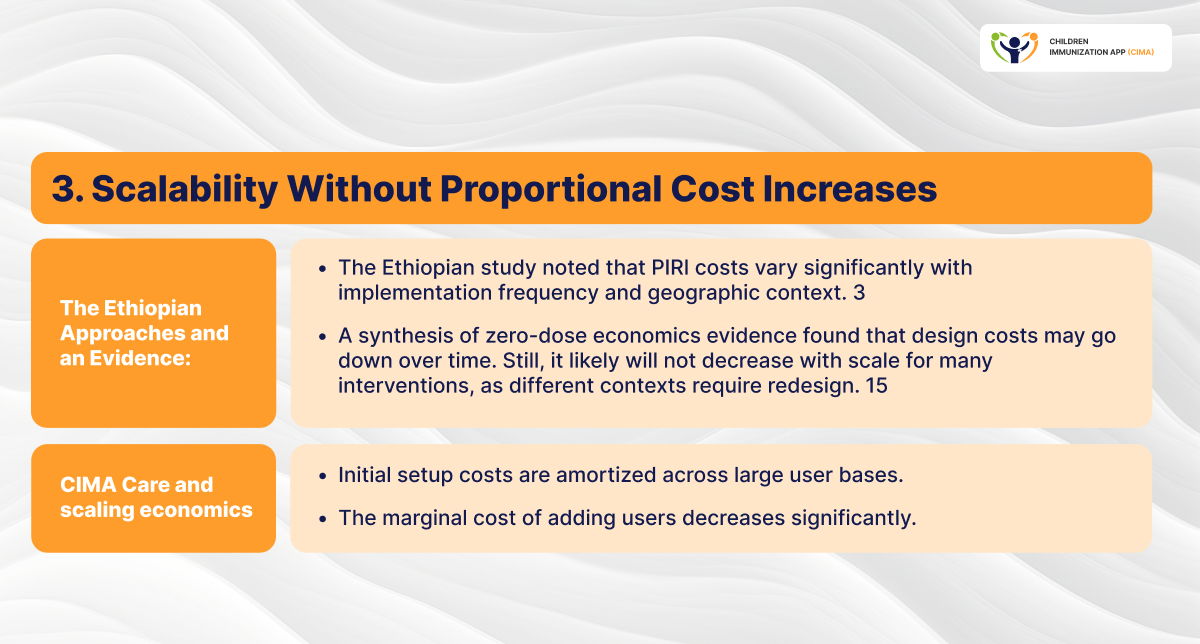
Scaling advantage: CIMA's marginal costs decrease while traditional approaches require redesign.
Integration efficiency: CIMA's $5.50 delivers immunization plus maternal & child health holistically.
Ethiopian study reveals integration & targeting principles that CIMA's $5.50 solution embodies.
Study confirms routine systems need tracking & collaboration—CIMA's $5.50 enables both digitally.
How CIMA's $5.50 delivers efficiency: real-time data, automated screening & gap identification.

CIMA's $5.50 tackles 6 Ethiopian barriers: mobility tracking, efficiency tools & automated education.
CIMA's $5.50 enhances all strategies: the digital backbone connecting campaigns, mobile & routine care.
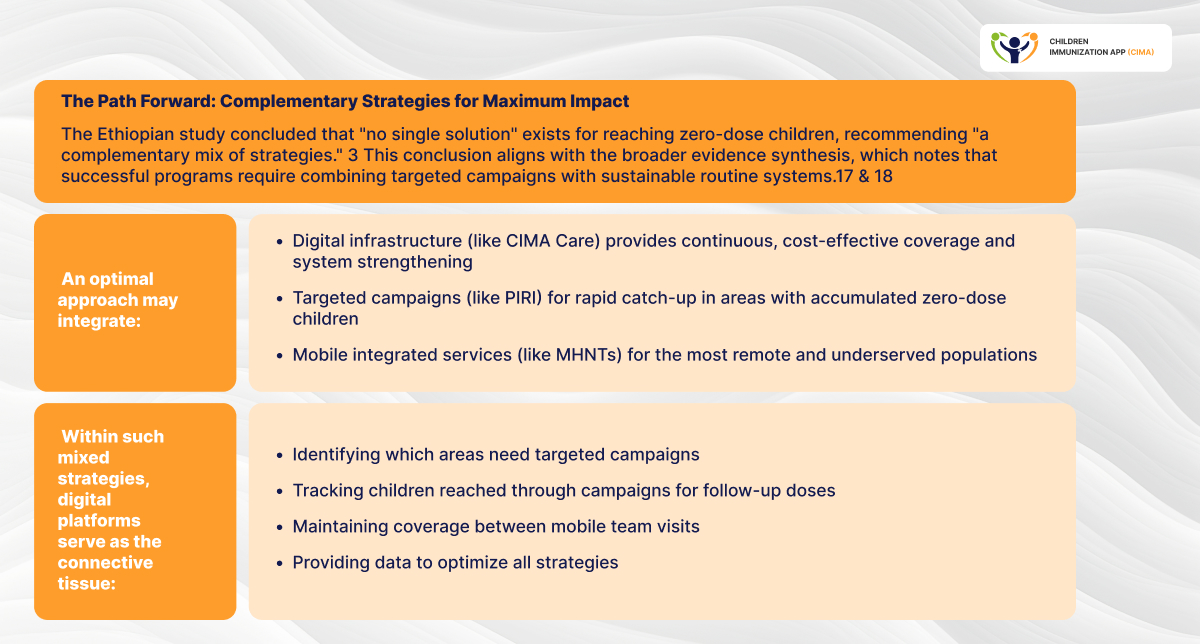
Conclusion: Cost-Effectiveness Through Comprehensive Solutions
The rigorous Ethiopian costing study provides invaluable evidence about the economics of reaching zero-dose children in challenging contexts. Its findings, that PIRI costs $6.65 per zero-dose child reached while routine services range from $52.47 to $90.40, establish important benchmarks for immunization delivery efficiency.
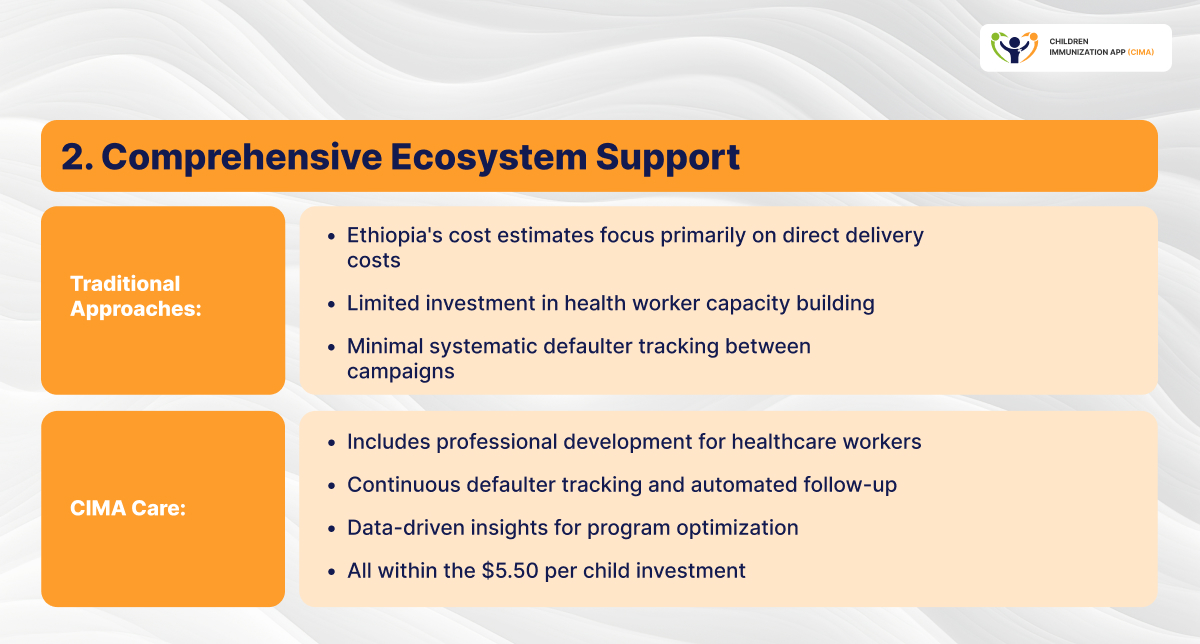
However, these figures also illuminate the critical importance of comprehensive, integrated approaches. CIMA Care's $5.50 per child investment delivers not just vaccination services, but a complete ecosystem of:
- Continuous engagement preventing children from becoming zero-dose
- Real-time tracking and defaulter identification
- Healthcare worker capacity building
- Data-driven program optimization
- Multi-stakeholder coordination
- Sustainable, scalable infrastructure
As the global health community works toward the Immunization Agenda 2030 goal of reaching every child with life-saving vaccines, evidence increasingly points toward integrated digital platforms as essential infrastructure, not replacing traditional delivery strategies but enhancing their effectiveness and efficiency while providing sustainable coverage between campaigns.
For health systems grappling with limited resources and substantial zero-dose populations, the question is not whether to invest in comprehensive digital solutions, but how quickly they can be implemented to prevent another generation of children from missing this critical protection.
CIMA's $5.50 enhances all strategies: the digital backbone connecting campaigns, mobile & routine care.
Learn More About CIMA Care
CIMA Care is actively supporting immunization programs in achieving equity and improved vaccination outcomes. To explore how CIMA Care's cost-effective, evidence-based platform can strengthen your immunization program:
Stay connected with us:
- 💼 LinkedIn: CIMA Care LinkedIn
- 🌐 Website: www.cima.care
- 📧 Email: support@cima.care
- 💬 WhatsApp: CIMA Health Academy | Official Updates | WhatsApp Channel
- 📱 CIMA App Manual: https://www.cima.care/CIMA-LMS-Manual2.pdf
Image References
- 1. Immunization Economics. Ethiopia study finds delivery cost per zero-dose child reached as low as $6.65 [Internet]. 2025 Nov 26 [cited 2026 May 28]. Available from: https://immunizationeconomics.org/recent-activity/2025/11/26/ethiopia-study-finds-delivery-cost-per-zero-dose-child-reached-as-low-as-6-65/
- 2. Adobe Stock. African woman show vaccine for Federal Democratic Republic of Ethiopia vaccination of Africa countries concept [Internet image]. [cited 2026 May 28]. Available from: https://stock.adobe.com/images/african-woman-show-vaccine-for-federal-democratic-republic-of-ethiopia-vaccination-of-africa-countries-concept/408526020
- 3. ResearchGate. The Cost of Reaching Zero-Dose Children in Ethiopia [Internet]. [cited 2026 May 28]. Available from: https://www.researchgate.net/publication/401424134_The_Cost_of_Reaching_Zero-Dose_Children_in_Ethiopia
- 4. CIMA Care. Media [Internet]. [cited 2026 May 28]. Available from: https://www.cima.care/media
- 5. Adobe Stock. Portrait of an African American woman and her family [Internet image]. [cited 2026 May 28]. Available from: https://stock.adobe.com/images/portrait-of-an-african-american-woman-and-her-family/314803619
- 6. Adobe Stock. Parents carrying son on shoulders on beach vacation [Internet image]. [cited 2026 May 28]. Available from: https://stock.adobe.com/images/parents-carrying-son-on-shoulders-on-beach-vacation/246367828
- 7. Adobe Stock. Young African American woman holding her baby's hand at home [Internet image]. [cited 2026 May 28]. Available from: https://stock.adobe.com/images/young-african-american-woman-holding-her-baby-s-hand-at-home/543224844
- 2. Author(s) unknown. Article available on PubMed Central [Internet]. PubMed Central; [cited 2026 May 26]. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC10050023/
- 3. CIMA Care. Stories [Internet]. CIMA Care; [cited 2026 May 26]. Available from: https://www.cima.care/insights/stories/
Blog Resources
- 1- drroopesh. WHO updates Fact Sheet on Immunization Coverage (15 July 2025) [Internet]. communitymedicine4all. 2025. Available from: https://communitymedicine4asses.wordpress.com/2025/07/18/who-updates-fact-sheet-on-immunization-coverage-15-july-2025/
- 2- Jarso H, Yohannes D, Gebru T, Kebebe L, Mengistu T, Tolera D, et al. Zero‐Dose Vaccination Among Children Aged 12–35 Months in Ethiopia. Mejía-Aranguré JM, editor. The Scientific World Journal [Internet]. 2025 Jan [cited 2025 Dec 2];2025(1). Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12657096/
- 3- The Cost of Reaching Zero-Dose Children in Ethiopia [Internet]. [cited 2025 Dec 2]. Available from: https://immunizationeconomics.org/wp-content/uploads/2025/11/Ethiopia-ZD-costing-study-report_final.pdf
- 4- Ingle EA, Shrestha P, Seth A, Lalika MS, Azie JI, Patel RC. Interventions to Vaccinate Zero-Dose Children: A Narrative Review and Synthesis. Viruses [Internet]. 2023 Oct 1;15(10):2092. Available from: https://www.mdpi.com/1999-4915/15/10/2092
- 5- What do we know about the economics of reaching zero-dose children? KEY TAKEAWAYS [Internet]. [cited 2025 Dec 2]. Available from: https://immunizationeconomics.org/wp-content/uploads/2025/10/Zero-dose-evidence-synthesis-17-October.pdf
- 6- Brief A. The Economics and Value of Immunizing Zero-Dose Children [Internet]. 2023. Available from: https://publichealth.jhu.edu/sites/default/files/2024-02/62-zd-and-economic-benefitsadvocacy-briefax.pdf
- 7- Wikipedia Contributors. Oromia. Wikipedia. Wikimedia Foundation; 2025.
- 8- Yayah Emerencia Ngah, George Ikomey Mondinde, Rasa Nikooifard, Cornelius Chebo, Shalom Tchokfe Ndoula, Ujjwal Neogi, Claudia Hanson, Tobias Alfven, Eresso Aga, Wadih Mallouf, Ziad El-Khatib. Enhancing vaccination uptake and parenting education through automated SMS service: A non-RCT pilot study in Bamenda, Cameroon. Mediterranean Life Sciences Union Annual Meeting (MedLIFE-24), Istanbul, Türkiye, December 2024.
- 9- El-Halabi S, Khader YS, Khdeir MA, Hanson C, Alfvén T, El-Khatib Z. Children immunization app (CIMA): A non-randomized controlled trial among Syrian refugees in Zaatari camp, Jordan. Journal of Prevention. 2023 Apr;44(2):239-52.
- 10- Soha El-Halabi, Khader Y, Mohammad Abu Khdeir, Hanson C, Alfvén T, Ziad El-Khatib. Children Immunization App (CIMA): A Non-randomized Controlled Trial Among Syrian Refugees in Zaatari Camp, Jordan. Journal of Prevention. 2023 Jan 17;44(2):239–52.
- 11- Khader Y, Maalouf W, Mohammad Abu Khdair, Mohannad Al-Nsour, Aga E, Khalifa A, et al. Scaling the Children Immunization App (CIMA) to Support Child Refugees and Parents in the Time of the COVID-19 Pandemic: A Social Capital Approach to Scale a Smartphone Application in Zaatari Camp, Jordan. 2022 Jan 3;12(1):7–12.
- 12- Yayah Emerencia Ngah, Ghazal Raoufi, Maral Amirkhani, Esmaeili A, Rasa Nikooifard, Shidrokh Ghaemimood, et al. Testing the Impact of Phone Texting Reminders for Children’s Immunization Appointments in Rural Cameroon: Protocol for a Nonrandomized Controlled Trial. JMIR Research Protocols. 2023 Aug 9;12:e47018–8.
- 13- A Year of Collective Action for Evidence-Based Drug Use Prevention [Internet]. United Nations: Office on Drugs and Crime. 2021. Available from: https://www.unodc.org/unodc/drug-prevention-and-treatment/news-and-events/2025/january/a-year-of-collective-action-for-evidence-based-drug-use-prevention.html
- 14- Li W, Sewolo F, Aoun A, Boltena MT, Musad A, Lindstrand A, Alfvén T, Hanson C, & El-Khatib Z. Characteristics of Studies Focusing on Vaccine Series Completion Among Children Aged 12–23 Months in Sub-Saharan Africa: A Scoping Review. Children. 2025;12(4):415.
- 15- WHY RESEARCH PRINCIPLES? [Internet]. [cited 2025 Dec 3]. Available from: https://immunizationeconomics.org/wp-content/uploads/2024/09/Research-principles-ZD-costing-2-Sept-2024.pdf
- 16- Eudes A, van, Bawa S, Balcha Masresha, Wagai J, Oteri J, et al. The cost of implementing a measles campaign in Nigeria: comparing the stand-alone and the integrated strategy. Health Economics Review [Internet]. 2023 Jun 13;13(1). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10262122/
- 17- SUPPLEMENTAL STRATEGIES TO REACH ZERO-DOSE CHILDREN JULY 2022 Scoping Review SUMMARY REPORT TO GAVI, ON BEHALF OF THE ZAMBIA EVALUATION & RESEARCH OF 0-DOSE (ZER0-D) PROJECT SCOPING REVIEW SUMMARY REPORT SUPPLEMENTAL IMMUNIZATION STRATEGIES TO REACH ZERO-DOSE CHILDREN BACKGROUND [Internet]. Available from: https://publichealth.jhu.edu/sites/default/files/2024-02/supplemental-strategies-gavi-zerod-scoping-reviewax.pdf
- 18- INTEGRATED CAMPAIGNS EVIDENCE BRIEF Evidence on pro-equity interventions to improve immunization coverage for zero-dose children and missed communities [Internet]. [cited 2025 Dec 3]. Available from: https://zdlh.gavi.org/sites/default/files/2023-09/7._integrated_campaigns_evidence_brief.pdf
- 19- CIMA Care. (2025). Cost-Effective Digital Solutions for Equitable Immunization Programs. Available from: https://www.cima.care/CIMA-Cost-Effective-Digital-Solutions-for-Equitable-Immunization-Programs.pdf
Enjoyed this article?
Share it with your friends on LinkedIn: Bridging the Immunization Gap: How Digital Innovation Delivers Cost-Effective Solutions for Zero-Dose Children![]()
Follow us on LinkedIn for more updates and insights: Cima Care GmbH ![]()